
Most healthcare practices treat new employee training like a one-week orientation followed by "figure it out as you go." Then six months later, you're dealing with billing errors, scheduling disasters, and patient complaints that all trace back to staff who never really learned their job properly.
Why training gaps quietly destroy clinic margins
The real problem isn't that new hires make mistakes. It's that those mistakes compound. A front desk coordinator who doesn't understand insurance verification creates downstream chaos for billing. A medical assistant who takes incomplete vitals forces providers to spend extra time with each patient. These small training gaps turn into operational hemorrhages that bleed profit and wreck patient experience.
Running a real clinic staff onboarding system means building competency checkpoints that actually prevent these failures before they happen—not hoping people pick things up over time, but systematically verifying they can perform every critical task to standard.
Why shadowing-based training almost always fails
Healthcare practices usually onboard staff through shadowing. Watch someone else do the job for a few days, maybe get a binder of policies nobody reads, then start working solo when things get busy. This approach basically guarantees inconsistency.
Eliminate appointment gaps and no-shows.
GoCliny streamlines every patient interaction from booking to billing—seamlessly.
- Unified appointment scheduling
- Automated patient reminders
- Staff calendar & task management
No credit card required
Different trainers emphasize different things. The morning shift front desk person teaches one way to handle prior authorizations. The afternoon shift teaches another. Neither gets documented. New hires pick up fragments of both and build their own hybrid process that probably misses critical steps.
The drift accelerates when practices grow. A single-provider clinic might survive informal training because everyone works closely together. But add a second location or grow to five providers, and suddenly you have staff operating completely differently across sites. Same EHR, same policies on paper, wildly different execution.
What makes this worse is that healthcare roles involve both technical skills and judgment calls. A medical assistant needs to know how to take blood pressure correctly (technical) but also when to alert the provider about concerning vitals (judgment). Traditional shadowing barely covers the technical parts and mostly ignores judgment training altogether.
The financial impact shows up everywhere—insurance claim denials because front desk staff didn't capture required information, patient no-shows because nobody explained the confirmation process properly, provider burnout from constantly re-explaining basic workflows. These aren't random failures. They're predictable outcomes of incomplete onboarding.
Building 30/60/90 day competency milestones that actually work
A functional clinic staff onboarding system breaks competency development into measurable phases. Not vague goals like "understand billing," but specific capabilities like "process three different insurance verification scenarios without assistance."
30-Day Milestones: Core Technical Skills
-
Complete patient check-in for 20 consecutive patients without errors
-
Process insurance verification for Medicare, commercial PPO, and HMO plans
-
Handle appointment scheduling across all provider templates
-
Execute proper phone etiquette scripts for 10 common scenarios
-
Navigate the EHR to find patient history, upcoming appointments, and billing status
For medical assistants, the 30-day targets focus on clinical basics:
-
Accurate vital signs collection verified against 15 patients
-
Proper room turnover meeting infection control standards
-
EHR documentation of chief complaints and medication lists
-
Basic supply inventory and restocking procedures
-
Emergency protocol awareness (not execution, just knowledge)
These aren't suggestions—they're pass/fail checkpoints. If someone can't meet these standards by day 30, you have a remediation decision to make immediately, not after they've spent another month developing bad habits.
60-Day Milestones: Workflow Integration
The second month shifts from isolated tasks to integrated workflows. Now you're testing whether staff can handle real-world complexity.
Front desk 60-day competencies:
-
Manage conflicting priorities (phone, walk-in, provider request simultaneously)
-
Handle billing inquiries and basic payment posting
-
Execute proper denial management workflows
-
Coordinate with clinical staff on patient flow
-
Identify and escalate urgent clinical situations using established triage protocols
Medical assistant 60-day competencies:
-
Independent room management for a half-day schedule
-
Accurate medication reconciliation with patient verification
-
Proper specimen handling and lab coordination
-
Basic procedure setup for common office procedures
-
Provider preference management across multiple physicians
At 60 days, you're looking for smooth execution under normal conditions. Staff should handle standard situations without constant supervision.
90-Day Milestones: Advanced Competency
By three months, staff should operate independently and handle exceptions. This is where you verify judgment alongside technical skill.
-
Handle an angry patient demanding an immediate appointment
-
Process a complex prior authorization with missing information
-
Manage a clinical emergency while providers are occupied
-
Resolve insurance coverage confusion with conflicting information
-
Train another staff member on a basic workflow
These scenarios test whether someone truly understands their role versus just following scripts. A front desk coordinator who can't explain why insurance verification matters will eventually skip steps when things get busy. A medical assistant who doesn't understand vital sign ranges won't recognize when something needs immediate attention.
Role-specific competency checklists that prevent gaps
Generic training checklists miss the nuances of healthcare roles. A billing specialist needs different competencies than a patient coordinator, even if both touch the revenue cycle.
Front Desk Competency Framework
Administrative competencies:
-
Insurance verification (5 carrier types minimum)
-
Prior authorization submission and tracking
-
Copay collection and payment posting
-
Appointment scheduling across provider types
-
Patient registration with demographic verification
Communication competencies:
-
Phone triage for clinical urgency
-
De-escalation techniques for upset patients
-
HIPAA-compliant information sharing
-
Provider communication protocols
-
Referral coordination with specialists
System competencies:
-
EHR navigation and documentation
-
Practice management software operation
-
Report generation for common requests
-
Portal message management
-
Equipment troubleshooting (printers, scanners, fax)
Medical Assistant Competency Framework
Clinical competencies:
-
Vital signs with manual backup methods
-
Medication administration (if authorized)
-
Phlebotomy and specimen collection
-
EKG and basic diagnostic tests
-
Infection control and PPE protocols
Administrative competencies:
-
Room flow management
-
Supply ordering and inventory
-
Chart preparation and review
-
Results communication to providers
-
Patient education documentation
Provider support competencies:
-
Procedure assistance and setup
-
Scribe functions (if applicable)
-
Prescription refill processing
-
Lab result preliminary review
-
Schedule optimization suggestions
Each competency needs specific verification criteria. "Knows how to take blood pressure" becomes "Demonstrates manual blood pressure on 5 patients with readings within 4 mmHg of automatic cuff."
Manager dashboards for tracking training progress
Tracking competency development across multiple new hires requires real visibility. A proper manager dashboard shows exactly where each trainee stands against their timeline.
The dashboard should display:
Individual Progress View:
-
Days in role vs milestone timeline
-
Completed competencies by category
-
Failed assessments requiring remediation
-
Scheduled upcoming evaluations
-
Trainer notes and observations
Cohort Analysis View:
-
Average time to competency by role
-
Common failure points across trainees
-
Trainer effectiveness comparison
-
Remediation success rates
-
Early termination patterns
Risk Indicators:
-
Trainees behind milestone schedule
-
Competencies with high failure rates
-
Trainers with poor success rates
-
Roles with extended time-to-productivity
-
Correlation between training gaps and operational issues
Manual tracking in spreadsheets breaks down quickly. You need systematic data collection that doesn't require managers to chase down information. When a trainer completes an assessment, it should immediately update the dashboard. When someone fails a competency check, it should trigger the remediation process.
Move medication reconciliation training to week three if trainees lack EHR familiarity to improve pass rates.
create an image depicting a workflow: trainer completes assessment on mobile device → dashboard updates trainee progress and flags failed competencies → remediation playbook is triggered and a re-assessment is scheduled
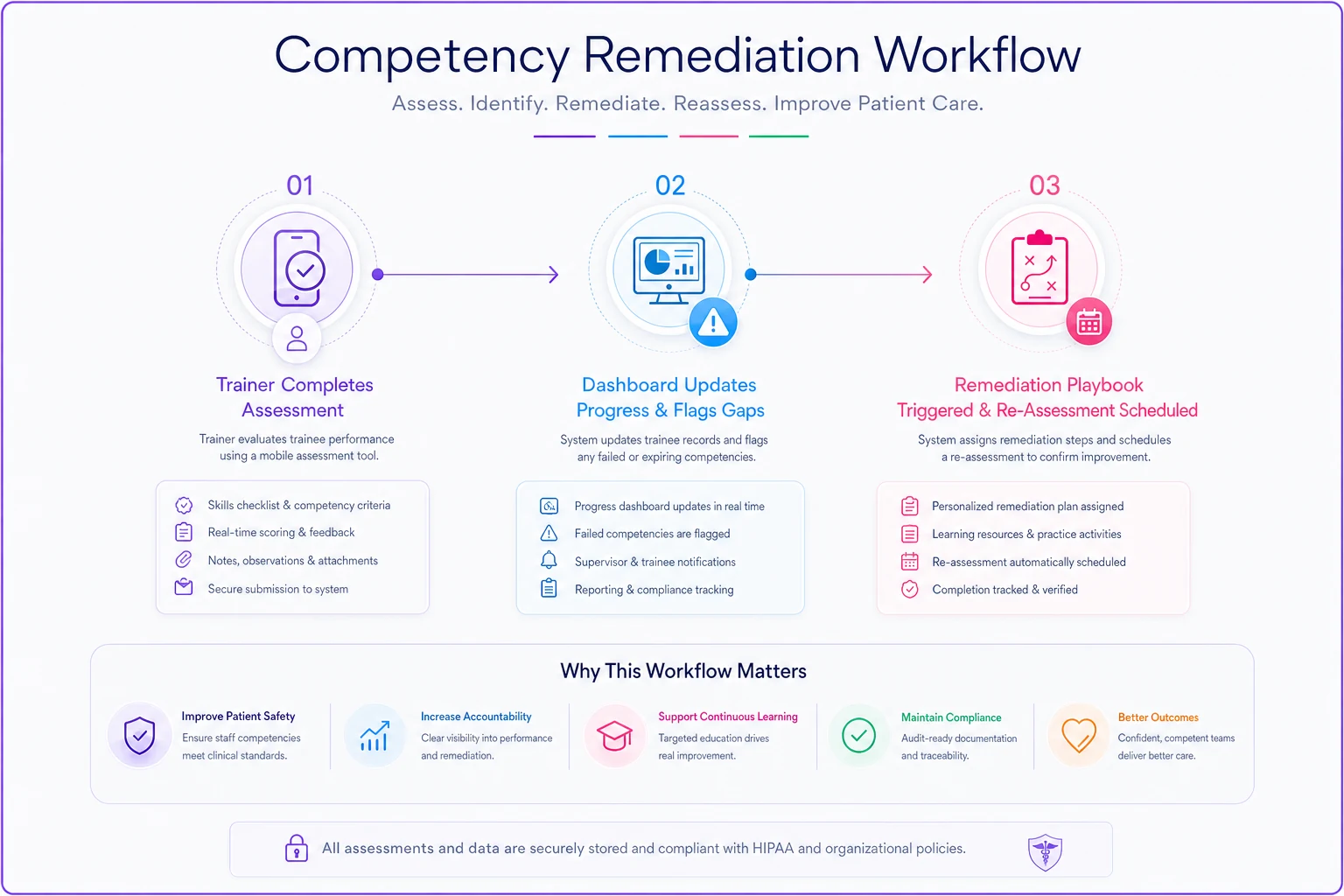
One orthopedic practice I worked with discovered their medical assistants consistently failed medication reconciliation competencies around day 45. The dashboard pattern revealed the issue: trainers were covering med rec in week one, before new hires understood the EHR well enough to retain the process. Moving that training to week three improved pass rates by roughly 40%.
Remediation playbooks for common competency failures
Not everyone learns at the same pace, and competency failures don't automatically mean termination. But you need structured remediation that addresses specific gaps without disrupting operations.
Remediation Trigger Protocol
-
Document the specific failure (not "bad at phones" but "couldn't transfer to voicemail")
-
Identify root cause (knowledge gap, skill gap, or performance issue)
-
Assign targeted remediation based on cause
-
Set remediation timeline (typically 5–7 business days)
-
Schedule re-assessment with a different evaluator
Knowledge Gap Remediation
-
Provide written materials or videos for self-study
-
Schedule a dedicated Q&A session with a subject expert
-
Create practice scenarios without patient impact
-
Test understanding before allowing patient interaction
Skill Gap Remediation
-
Increase supervised repetition
-
Break complex tasks into smaller components
-
Pair with a high-performing peer for modeling
-
Use simulation or role-play for practice
Performance Issue Remediation
-
Review environmental factors (too many simultaneous tasks?)
-
Assess motivation and engagement
-
Implement performance monitoring with immediate feedback
-
Consider role fit evaluation
The remediation playbook should specify exactly how many attempts someone gets before termination. Typically: two remediation cycles for 30-day competencies, one cycle for 60-day competencies, and case-by-case evaluation for 90-day competencies.
Preventing operational drift through standardized shadowing
Shadowing is still valuable for healthcare training, but only when standardized. Random shadowing where new hires follow whoever's available creates more problems than it solves.
Shadowing Scripts
-
Create actual scripts for trainers covering what to explain during common tasks. When processing a prior authorization, the trainer should cover:
-
- Why this prior auth is needed
-
- Where to find insurance requirements
-
- What information commonly causes delays
-
- How to track submission and follow-up
-
- When to escalate to management
Without scripts, trainers focus on different aspects based on their own experience. One might emphasize speed, another accuracy—new hires absorb conflicting messages and end up somewhere in between, usually missing critical steps.
Progressive Independence Protocol
-
Days 1–3
Pure observation with note-taking
-
Days 4–7
Explain what you would do before trainer acts
-
Days 8–10
Perform simple tasks with trainer watching
-
Days 11–14
Handle routine workflows with trainer nearby
-
Day 15+
Independent work with scheduled check-ins
Trainer Certification
-
Demonstrate consistent performance above standards
-
Complete a train-the-trainer workshop
-
Practice with HR or management observation
-
Maintain training quality metrics
Bad trainers create bad employees. One family practice I know traced their highest front desk turnover back to a single trainer who openly complained about the job throughout shadowing. New hires absorbed the negativity and either quit early or developed the same attitude. Nobody caught it for nearly a year.
The hidden costs of inconsistent onboarding
Poor onboarding costs more than just training time. The downstream impacts compound across your entire operation.
Revenue Impact
| Issue | Root Cause |
|---|---|
| Insurance claim denials | Eligibility verification errors |
| Provider downtime | Scheduling mistakes |
| Missing charges | Improper documentation |
| Copay collection failures | Unclear protocols |
| Patient attrition | Poor service experiences |
A multi-site urgent care chain tracked error rates by employee tenure and found staff with incomplete onboarding generated roughly 3x more billing errors in their first year compared to properly trained colleagues. At around $150 per denied claim requiring rework, each poorly trained employee cost them close to $2,800 annually in billing labor alone.
Quality and Compliance Risk
-
HIPAA violations from improper information handling
-
Clinical errors from inadequate vital sign training
-
Infection control breaches from missed protocols
-
Documentation gaps creating legal liability
-
Patient safety events from poor communication
Team Morale Destruction
Experienced staff resent constantly fixing new employee mistakes. Providers lose patience re-explaining the same workflows. Good employees leave because they're exhausted working alongside colleagues who never improve.
The morale impact often exceeds the financial cost. When your best medical assistant quits because they've been quietly compensating for undertrained coworkers for months, you've lost institutional knowledge no onboarding system can quickly replace.
Technology integration for scalable competency tracking
Paper checklists and spreadsheets can't scale across multiple locations or dozens of employees. Modern clinic staff onboarding systems need technology infrastructure that automates tracking without creating administrative burden.
Digital Competency Verification
-
Mobile-friendly assessment forms trainers complete in real-time
-
Photo or video verification for complex procedures
-
Electronic signatures with timestamps
-
Automatic escalation when milestones are missed
-
Integration with HR systems for compliance tracking
Automated Reporting and Alerts
-
Day 25 warning if 30-day competencies aren't progressing
-
Trainer notification when assessment is due
-
Management escalation for failed remediation
-
Monthly dashboard updates showing training program health
Knowledge Base Integration
-
Training videos for each competency
-
Written protocols and job aids
-
Update notifications when procedures change
-
Performance support tools for reference
-
Searchable database of common questions
AI-powered operational software helps especially with pattern recognition across training cohorts. When multiple trainees fail the same competency, the system surfaces curriculum gaps. When certain trainers consistently produce strong graduates, it highlights what they're doing differently.
One pediatric practice implemented digital competency tracking and discovered their insurance verification process had 14 undocumented steps that experienced staff did automatically but never formally taught. Building those steps into the training reduced verification errors by around 60% within two months.
Building feedback loops between training and operations
Your clinic staff onboarding system should continuously improve based on operational outcomes. Connect training metrics to business performance to identify what actually matters.
Correlation Analysis
-
Specific competency scores and error rates
-
Training completion time and productivity metrics
-
Trainer quality and employee retention
-
Remediation needs and eventual performance
-
Onboarding approach and patient satisfaction scores
Continuous Curriculum Refinement
-
Billing denials → Which verification competency was missed?
-
Patient complaints → Which service competency needs reinforcement?
-
Provider frustration → Which clinical competency requires updating?
-
Scheduling chaos → Which workflow competency lacks clarity?
Competency Expiration and Refreshers
-
Emergency procedures (annual recertification)
-
Rarely-used insurance protocols (semi-annual review)
-
Specialty-specific workflows (quarterly validation)
-
Compliance requirements (per regulatory schedule)
Skills decay without practice. Implement competency expiration for critical but infrequent tasks.
Making the investment case for systematic onboarding
The ROI on comprehensive onboarding seems intangible until you actually run the numbers.
Direct Cost Savings
-
Reduced overtime from competent staff working efficiently
-
Lower error-related rework costs
-
Decreased recruitment costs from better retention
-
Reduced training redundancy from standardization
-
Fewer compliance penalties from proper protocols
Productivity Acceleration
| Approach | Average Timeline |
|---|---|
| Traditional shadowing-based onboarding | 4–6 months |
| Systematic competency-based onboarding | 60–90 days |
| Value of accelerated productivity | 2–3 months additional capacity |
For a medical assistant earning $18/hour, reaching full productivity 60 days faster saves roughly $5,800 in underutilized wages per hire.
Risk Mitigation Value
| Risk Event | Estimated Cost |
|---|---|
| Significant billing error | $2,000–$5,000 |
| HIPAA violation | $50,000+ |
| Patient safety event | $25,000–$100,000 |
| Provider turnover from staff incompetence | $80,000–$150,000 |
Even preventing one moderate incident per year justifies the entire onboarding investment.
Systematic competency as a competitive advantage
Strong healthcare practices don't succeed through heroic individual efforts. They build systems that consistently produce competent staff who execute reliably. A real clinic staff onboarding system becomes the foundation for operational stability.
Practices struggling with constant fires, staff turnover, and patient complaints almost always trace back to training gaps. Someone didn't learn their job properly, that gap created downstream problems, and now everyone's in crisis mode trying to compensate.
Practices with systematic onboarding operate differently. New hires reach competency on a predictable timeline. Mistakes get caught early through milestone assessments. Remediation happens before bad habits form.
The 30/60/90 day framework with role-specific competencies isn't micromanagement—it's giving every employee a real shot at succeeding. When people know exactly what's expected and receive proper training to meet those expectations, they perform better and stay longer.
Building this requires upfront investment in documenting competencies, training trainers, and implementing tracking technology. The alternative is perpetual operational drift where quality depends on individual heroics rather than repeatable systems.
For practices serious about scaling past founder dependency or single-site limitations, competency standardization isn't optional. It's the difference between a practice that muddles through and one that delivers consistent, profitable care regardless of who's working that day.
Ready to transform your practice workflow?
Join 2,000+ healthcare providers using GoCliny to increase efficiency, improve patient satisfaction, and grow revenue.