

Three months back, a dermatology practice in Phoenix showed me their "comprehensive" monthly operational dashboard healthcare setup. Twenty-seven metrics tracked across six different spreadsheets. Color-coded heat maps. Automated email reports every Monday morning.
Their front desk coordinator spent four hours every month pulling numbers. The practice manager reviewed everything in a monthly meeting. Everyone nodded. Nothing changed.
The problem wasn't the metrics. It was the disconnect between numbers on a screen and actual operational decisions. They were tracking appointment volume but nobody owned the response when it dropped. They monitored patient wait times but had no protocol for when thresholds got crossed. The dashboard became expensive wallpaper — pretty to look at, meaningless for operations.
After rebuilding their entire approach, that same practice now runs on just eight core KPIs. Each metric has an owner. Every threshold triggers a specific action. Their operational meetings dropped from two hours to thirty minutes because everyone knows exactly what needs doing before they walk in the room.
Why traditional healthcare dashboards fail
Most healthcare practices build dashboards backwards. They start with what's easy to measure, not what actually drives operational decisions.
You probably track total patient visits, revenue per provider, maybe some appointment metrics. These numbers tell you what happened. They don't tell you what to do about it.
The real failure happens in the gap between measurement and action. A typical scenario: your dashboard shows patient volume dropped 12% last month. The practice manager mentions it in a meeting. Someone suggests "marketing more." The conversation moves on. Next month, volume is down another 8%.
What went wrong? No clear ownership. No predetermined response. No action threshold. The metric became a discussion topic instead of an operational trigger.
Traditional dashboards also suffer from metric overload. When you track everything, you optimize nothing. That dermatology practice? Of their original 27 metrics, only three actually influenced operational decisions. The rest was noise disguising itself as insight.
Building KPIs that trigger action
Effective KPIs in healthcare need three components most practices miss: explicit thresholds, designated owners, and predetermined responses.
Eliminate appointment gaps and no-shows.
GoCliny streamlines every patient interaction from booking to billing—seamlessly.
- Unified appointment scheduling
- Automated patient reminders
- Staff calendar & task management
No credit card required
Start with threshold design. Generic benchmarks don't work because every practice operates differently. A family medicine clinic might panic when same-day appointments drop below 15% of daily capacity. An endocrinology practice might run fine at 5%. Your thresholds need to reflect your specific operational reality.
One multi-specialty group built their threshold system like this:
Patient Access Metrics
-
Third-next-available appointment > 14 days = Yellow alert
-
Third-next-available appointment > 21 days = Red alert
-
New patient wait time > 30 days = Red alert
Financial Health Metrics
-
Collection rate < 94% = Yellow alert
-
Days in A/R > 35 = Yellow alert
-
Prior auth approval rate < 85% = Red alert
Operational Efficiency Metrics
-
Provider utilization < 75% = Yellow alert
-
No-show rate > 8% = Yellow alert
-
Patient cycle time > 65 minutes = Red alert
These aren't industry averages. They built thresholds based on their own operational breaking points — the moments when inefficiency starts costing real money or losing patients.
The action-mapping framework
Thresholds without actions are just colorful warnings. You need explicit protocols that kick in automatically when metrics cross lines.
An orthopedic practice in Dallas showed me their action-mapping system. Every KPI threshold links to a specific operational response:
No-show rate exceeds 8%:
-
Day 1
Front desk lead pulls no-show report by provider
-
Day 2
Identify patterns (time slots, patient types, insurance)
-
Day 3
Implement targeted reminder protocol
-
Day 7
Review effectiveness, adjust approach
Collection rate drops below 94%:
-
Immediate
Billing manager audits denial reasons
-
Within 48 hours
Staff retraining on problem codes
-
Within 1 week
Review payer contract terms
-
Within 2 weeks
Implement process changes
These aren't suggestions. They're operational requirements triggered automatically by the metrics. No meetings needed to decide if action is necessary. The threshold decides.
Here's a visual of the action-mapping workflow.
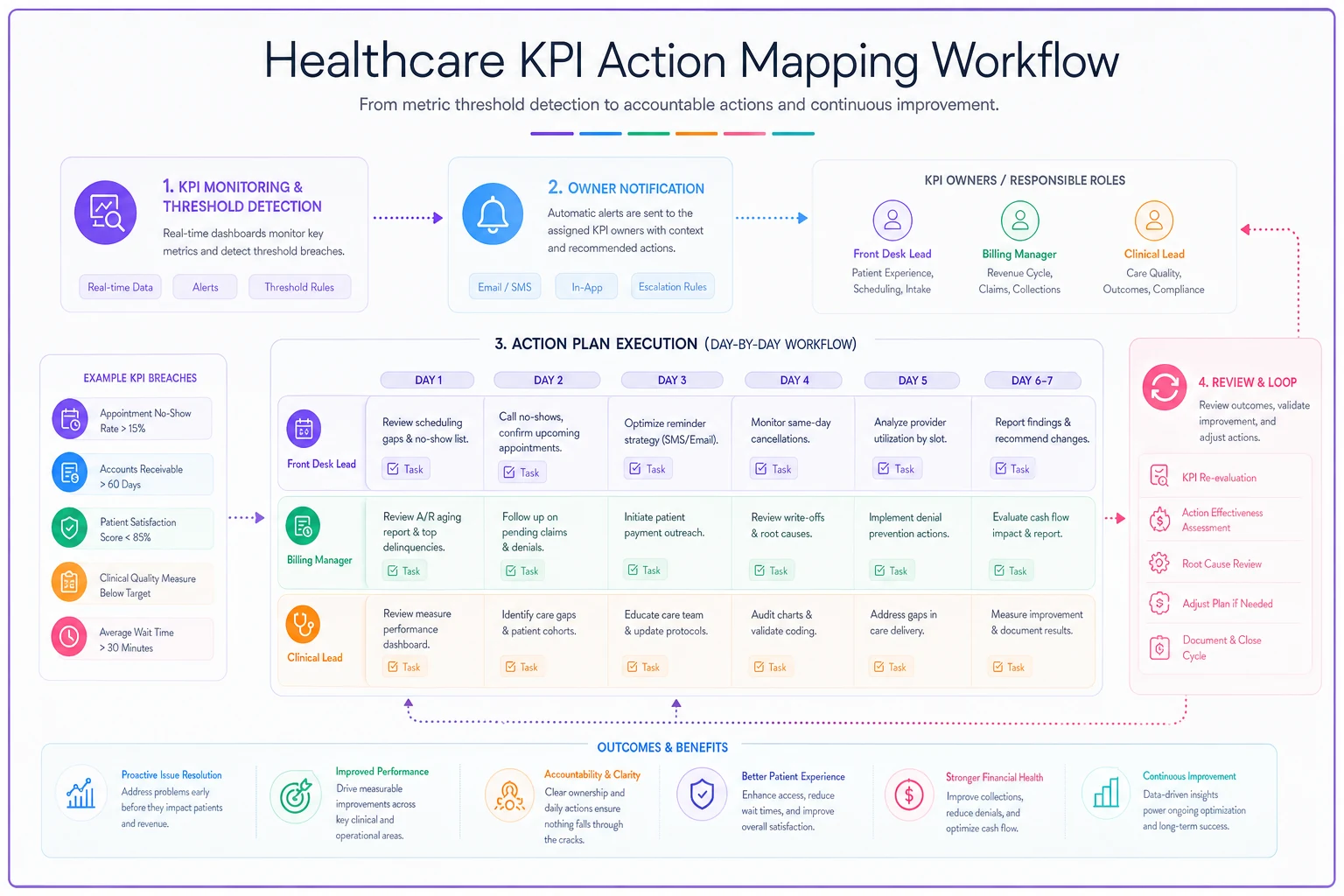
The graphic shows how a threshold breach moves from detection to assigned actions and review.
Sample dashboard design
Forget pretty visualizations. Your monthly operational dashboard healthcare system needs functional clarity above aesthetic appeal.
| KPI | Current | Threshold | Status | Owner | Triggered Action |
|---|---|---|---|---|---|
| Days to 3rd Available | 18 | >14 days | 🟡 | Schedule Manager | Add evening slots |
| Collection Rate | 92.3% | <94% | 🔴 | Billing Lead | Denial audit protocol |
| No-Show Rate | 6.8% | >8% | 🟢 | Front Desk Supervisor | Standard monitoring |
| Provider Utilization | 71% | <75% | 🟡 | Practice Manager | Template review |
| Patient Cycle Time | 58 min | >65 min | 🟢 | Clinical Lead | Standard monitoring |
| Prior Auth Approval | 83% | <85% | 🔴 | Auth Specialist | Payer escalation |
| Same-Day Availability | 11% | <15% | 🟡 | Schedule Manager | Buffer adjustment |
| A/R Days | 31 | >35 days | 🟢 | Billing Lead | Standard monitoring |
Simple. Clear. Actionable. No interpretation needed.
The status indicators (🟢🟡🔴) create visual hierarchy without complexity. Green means monitor. Yellow means investigate. Red means execute the predetermined response immediately.
Creating your action log template
Documentation beats memory. You need a system that tracks what actions were taken, by whom, and what happened next.
Action Log Entry Format:
-
Trigger Date
[When threshold was crossed]
-
Metric
[Which KPI triggered action]
-
Threshold Crossed
[Specific number/percentage]
-
Owner Notified
[Name and timestamp]
-
Action Taken
[Specific steps implemented]
-
Resources Used
[Staff hours, system changes, costs]
-
Result Check Date
[When to measure impact]
-
Outcome
[Measurable result after action]
Real example from their log:
Trigger Date: March 4 Metric: New patient wait time Threshold Crossed: 32 days (threshold: 30) Owner Notified: Sarah Chen, March 4, 9:15 AM Action Taken: Opened 2 additional new patient slots per provider per week, added Saturday morning clinic 2x monthly Resources Used: 16 additional provider hours monthly, 1 additional MA Saturday shift Result Check Date: March 18 Outcome: Wait time reduced to 24 days, maintained through April
This isn't busywork. It's institutional memory. Six months later when the same issue resurfaces, you know exactly what worked before.
Assigning ownership that sticks
KPI ownership fails when it's vague or spread across multiple people. "The team" never fixes anything. A specific person does.
Successful practices assign KPI ownership based on operational control, not organizational hierarchy. Your medical director probably shouldn't own front desk metrics. Your billing supervisor shouldn't own clinical efficiency scores.
-
Scheduling metrics → Scheduling coordinator (not practice manager)
-
Clinical efficiency → Lead nurse or MA (not providers)
-
Revenue cycle metrics → Billing supervisor (not CFO)
-
Patient satisfaction → Patient experience lead (not medical director)
Limit each owner to 2-3 KPIs so they can manage alerts and respond quickly.
One internal medicine practice had their practice manager listed as owner for 12 different KPIs. Impossible to manage effectively. After redistribution, each person owned 2-3 metrics maximum. Response time to threshold alerts dropped from days to hours.
Making monthly reviews actually matter
Monthly KPI reviews usually die from one of two causes: they become status update meetings or they turn into blame sessions. Neither drives operational improvement.
Pre-meeting requirements:
-
All threshold breaches already have actions in progress
-
Owners submit one-paragraph status for their metrics
-
Historical trends pulled for any metric showing 2+ months of decline
Meeting agenda (30 minutes max):
-
Red alerts only (5 minutes) - confirm actions are working
-
Pattern identification (10 minutes) - what's causing multiple yellows?
-
Resource allocation (10 minutes) - what support do owners need?
-
Next month's focus (5 minutes) - pick one metric to improve
No presentations. No defending numbers. No lengthy explanations. The dashboard already told the story. The meeting is for operational problem-solving only.
Common implementation failures
Too many metrics too fast. A cardiology practice tried launching with 15 KPIs simultaneously. Chaos. Start with 3-5 core metrics. Add others only after the first set runs smoothly for two months minimum.
Threshold paralysis. Setting thresholds too tight creates constant false alarms. Too loose and nothing ever triggers. Start conservative and tighten based on actual operational capacity. That orthopedic group? They adjusted thresholds four times in the first year before finding the right balance.
Action plans without resources. Telling someone to "reduce no-shows" without giving them tools or time guarantees failure. Every action plan needs allocated resources — whether that's staff hours, technology investment, or process change authority.
Ownership without authority. Your front desk lead can't fix prior authorization delays if they can't change workflows or reassign staff. Match ownership with operational control or the whole system breaks down.
Technology and automation considerations
Manual dashboard updates kill momentum. By the time you've compiled last month's numbers, you're already halfway through the current month.
Modern practice management systems can automate most KPI tracking, but the setup requires thoughtfulness. Don't just accept default reports. Configure triggers and alerts that match your specific thresholds.
Some practices use AI-powered operational software to automatically flag threshold breaches and initiate action protocols. The system sends alerts to designated owners, tracks response times, and documents actions taken. This removes the human delay between problem identification and response initiation.
The automation doesn't replace human judgment — it accelerates the response cycle. Instead of waiting for a monthly review to discover problems, issues surface immediately when thresholds break.
For practices still on legacy systems, even basic automation helps. Email alerts for threshold breaches. Automated report generation. Calendar reminders for action deadlines. Small automations compound into significant operational improvements.
When this approach doesn't work
You need stable operations first. If you're in crisis mode — providers quitting, systems failing, cash flow problems — fix those before implementing structured KPIs. Dashboards don't solve chaos; they optimize functioning systems.
Small practices might need modification. A three-provider practice can't assign dedicated owners to eight different metrics. Consolidate to 3-4 critical KPIs with shared ownership or rotating responsibility.
Seasonal practices require different thresholds. Pediatric practices see massive volume swings around school schedules. Dermatology spikes in summer. Static thresholds don't work when your baseline shifts predictably. Build seasonal threshold variants or use rolling averages.
Multi-site operations need centralized coordination. Individual site dashboards create competing priorities. Build a unified dashboard with site-specific drill-downs, but keep core KPIs consistent across locations.
Building momentum from metrics
Practices succeeding with this approach share one characteristic: they treat their dashboard as an operational tool, not a reporting requirement.
Your monthly operational dashboard healthcare system should drive decisions, not document them. Every metric needs a purpose. Every threshold needs an owner. Every breach needs a response.
Start small. Pick three KPIs that directly impact patient access or revenue. Assign clear owners. Design simple thresholds. Document every action and outcome. Build credibility through small wins before expanding the system.
Within three months, you'll notice the shift. Meetings become shorter because decisions are pre-made by thresholds. Problems get solved faster because ownership is clear. Performance improves because actions are consistent and documented.
The dashboard stops being something you review and becomes something you operate from. That's when metrics actually start moving the needle.
Ready to transform your practice workflow?
Join 2,000+ healthcare providers using GoCliny to increase efficiency, improve patient satisfaction, and grow revenue.