

Monday morning, 7:48 AM. Your practice manager texts the group chat: "Dr. Martinez called out sick, who can cover her 14 appointments today?" The cascade starts immediately. Your NP is already double-booked at the south location. The PA who could help is stuck doing procedures until 3 PM. Two providers volunteer partial coverage but now you're playing schedule Tetris across three locations while patients are already checking in.
This scenario destroys practices through slow erosion of provider satisfaction, patient trust, and operational efficiency. The real damage happens afterward—providers working through lunch, appointments running 45 minutes behind, staff fielding angry calls, and that underlying tension that makes everyone dread Mondays.
Most multi-provider clinics treat capacity planning like weather forecasting—something you check daily and hope for the best. They rely on scheduling software to flag conflicts, assume providers will speak up when overwhelmed, and cross their fingers that coverage gaps won't coincide with busy periods. This reactive approach might work when you have three providers in one location. Scale to 8+ providers across multiple sites, and you're managing a complex operational system that requires actual planning infrastructure.
The math is brutal. A six-provider practice with poor capacity planning loses roughly $7,000-8,000 monthly in unfilled slots due to coverage gaps. Add provider overtime from schedule chaos ($5,000 monthly), patient leakage from scheduling friction (5% annually, worth $500k+ over three years), and eventual turnover costs ($250k-500k per provider), and you're looking at operational bleeding that kills practices slowly but surely.
Why scheduling software fails at multi-provider scale
Traditional scheduling treats capacity planning as a booking problem rather than resource allocation. Your software shows when people are working but doesn't reveal whether capacity matches demand, whether coverage patterns create bottlenecks, or whether specific provider combinations stress the system.
The complexity isn't just mathematical—it's behavioral. Dr. Johnson prefers morning slots but will work evenings at the main location only. Your pediatric NP handles general appointments but needs 45-minute slots for ADHD evaluations. The new PA is qualified for minor procedures but requires supervision for three months.
Even sophisticated healthcare systems focus on booking efficiency rather than capacity optimization. They'll prevent double-booking the same provider but won't warn you that scheduling Dr. Chen for procedures Tuesday afternoons means no Spanish-speaking provider during peak walk-in hours.
Add multiple locations and you're managing:
-
Provider preferences for locations and schedules
-
Appointment types and durations by specialty
-
Different patient volumes at each site
-
Equipment and room constraints
-
Support staff allocation
-
Coverage for planned and unplanned absences
These constraints layer until scheduling becomes weekly negotiation rather than systematic process.
Building a monthly capacity planning system
You need systematic capacity planning that treats provider time as finite resource requiring active management. Not more scheduling software or buffer providers.
Eliminate appointment gaps and no-shows.
GoCliny streamlines every patient interaction from booking to billing—seamlessly.
- Unified appointment scheduling
- Automated patient reminders
- Staff calendar & task management
No credit card required
Monthly Planning Cadence
Run capacity planning on the third Thursday of each month for the following month. This timing provides enough lead time to adjust schedules and communicate changes while maintaining accuracy. The session takes 90-120 minutes with your practice manager, lead provider, and operations coordinator. Compare two hours of planning against the 15-20 hours you currently spend weekly fighting scheduling fires.
Here's a simple workflow to run the monthly planning session.
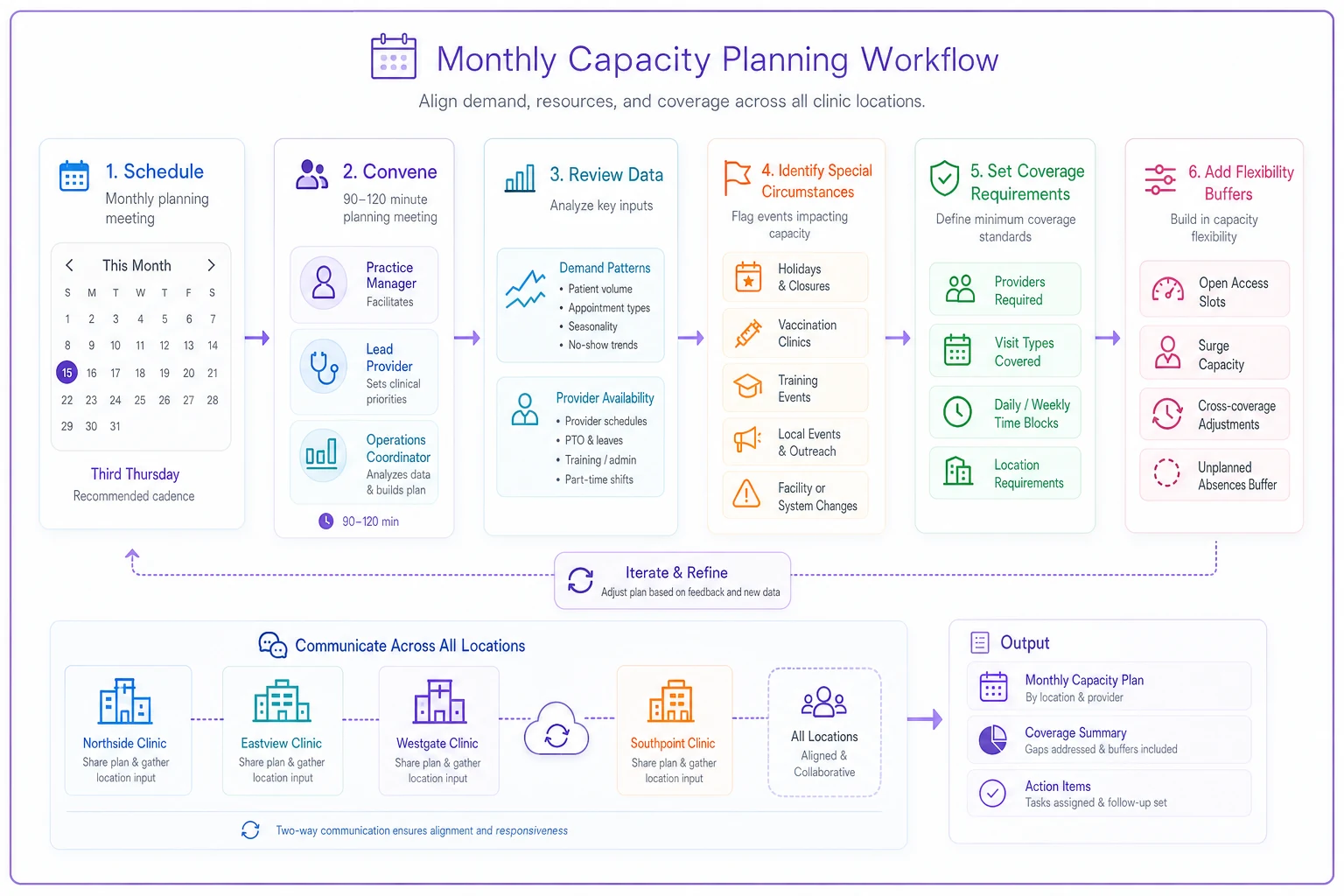
Hold the session on a consistent weekday so providers can plan around it and ensure steady attendance.
During this session, evaluate five core elements:
Demand patterns from the previous month—not just total volume, but distribution by type, time, location, and provider preference. Look for patterns like "Tuesday afternoons at the west clinic consistently run 20% below capacity" or "new patient physicals cluster on Mondays and Fridays."
Provider availability including scheduled time off and predictable patterns. Dr. Williams might be technically available Wednesdays but you know she's exhausted from hospital rounds the night before.
Special circumstances for the upcoming month. School physicals in August, flu shot campaigns in October, conferences that remove three providers simultaneously, Medicare wellness visit deadlines in December.
Coverage requirements by role and location—not just warm bodies in exam rooms but appropriate clinical coverage for different appointment types, administrative oversight at each location, and support staff ratios preventing bottlenecks.
Flexibility buffers for the unexpected, because someone will get sick and emergencies will happen. The question is whether you've built systematic resilience or you're hoping for luck.
Cross-coverage matrices that prevent cascade failures
The most powerful capacity planning tool is a well-designed cross-coverage matrix. Not a simple grid showing who covers whom, but a comprehensive map of capabilities, constraints, and optimal coverage patterns preventing single points of failure.
Create role-based coverage pools instead of thinking "Dr. Martinez covers for Dr. Johnson." Your "Complex Care Pool" might include two physicians and an experienced NP handling complicated chronic disease management. Your "Procedure Pool" includes anyone certified for minor surgeries. Your "Pediatric Pool" covers providers comfortable with children under five.
Within each pool, establish primary and secondary coverage relationships. Primary coverage means dropping everything to help when needed. Secondary coverage means available if primary is also out or overwhelmed. This hierarchy prevents the common scenario where everyone assumes someone else will handle it.
Coverage Priority Matrix Example
| Provider | Primary Coverage Pool | Secondary Pool | Location Flexibility | Time Flexibility |
|---|---|---|---|---|
| Dr. Chen (MD) | Complex Care, Procedures | Urgent Care | All locations | Can extend PM only |
| Dr. Williams (MD) | Complex Care, Pediatrics | Procedures | Main, North | Full flexibility |
| Sarah NP | Urgent Care, Pediatrics | Complex Care | All locations | No evenings |
| Mike PA | Procedures, Urgent Care | — | Main only initially | Can start early |
| Dr. Kumar (MD) | Complex Care | Urgent Care, Procedures | Main, South | Thursday PM unavailable |
| Jennifer NP | Pediatrics, Urgent Care | — | North, South | Mornings preferred |
When Dr. Williams calls out sick Tuesday morning at North clinic, you immediately know Sarah NP is primary coverage for pediatric appointments, Mike PA can handle procedures if supervised, and Dr. Chen could extend her afternoon for complex cases.
Forecasting templates that predict demand patterns
Most practices either don't forecast or use historical averages missing crucial patterns. Effective forecasting requires templates capturing both predictable patterns and seasonal variations while remaining simple enough to actually use.
Track three metrics weekly:
-
Appointment requests by type and urgency
-
Actual appointments completed
-
Turned away or rescheduled requests due to capacity
The gap between requests and completed appointments shows your true capacity constraint. If you're consistently turning away 20+ weekly requests while showing 15% no-show rates, you don't have a demand problem—you have scheduling inefficiency better capacity planning could solve.
Build separate forecasts for different appointment types. A 15-minute medication follow-up has completely different capacity implications than a 45-minute new patient evaluation.
| Appointment Type | Historical Weekly Average | Seasonal Adjustment | Projected Demand | Required Provider Hours | Current Allocated Hours | Gap |
|---|---|---|---|---|---|---|
| New Patient Physical | 32 | +20% (school season) | 38 | 38 hours | 42 hours | OK |
| Follow-up Visit | 156 | Baseline | 156 | 39 hours | 36 hours | -3 hrs |
| Urgent Care | 89 | +15% (flu season) | 102 | 34 hours | 30 hours | -4 hrs |
| Procedures | 18 | Baseline | 18 | 18 hours | 20 hours | OK |
| Wellness Visits | 44 | +30% (Q4 Medicare) | 57 | 28.5 hours | 24 hours | -4.5 hrs |
The seasonal adjustment column requires experience. August needs more capacity for school physicals. December sees wellness visit spikes as patients hit deductibles. April brings allergy-related urgent visits. These patterns repeat annually but most practices scramble each time.
Track provider productivity variations too. Dr. Kumar might average 18 patients daily while Jennifer NP sees 24, but if Dr. Kumar handles complex cases requiring longer visits, revenue per hour might be comparable.
Role-based shift rules preventing burnout
Treating all clinical hours as interchangeable burns out providers and creates chaos. A physician working urgent care 8 AM to noon shouldn't immediately flip to complex chronic disease management that afternoon. An NP covering three locations in one week will make more mistakes than one with stable site assignment.
Establish clear shift rules balancing operational needs with human limitations:
Maximum Consecutive Clinical Hours
-
Standard appointments
4 hours without 30-minute break
-
Urgent care
3 hours without break
-
Procedures
2.5 hours without break
After three hours of back-to-back urgent care visits, decision fatigue sets in. Error rates increase, patient satisfaction drops, providers cut documentation corners. That 30-minute break prevents the 2-hour end-of-day scramble fixing mistakes and completing notes.
Location Stability Requirements
-
Minimum 2 consecutive days at same location
-
Maximum 2 locations per week for any provider
-
Travel time counts as non-clinical administrative time
When providers bounce between locations daily, they lose efficiency from unfamiliar layouts, different support staff, varied patient populations. A provider who knows where supplies are kept and how patient flow works will see 20% more patients with less stress.
Coverage Balance Rules
-
No provider covers more than 2 weekends monthly
-
After emergency coverage, provider gets priority for next scheduling preference
-
Extended hours rotate monthly, not weekly
These prevent the scenario where flexible providers get exploited until they're not flexible anymore. Dr. Chen might willingly stay late today, but if she's always staying late, that willingness evaporates.
Technology integration enhancing human judgment
Modern capacity planning requires technological support without full automation. You need systems enhancing human decision-making rather than replacing it. The most effective approach combines automated data collection with human interpretation and adjustment.
Your scheduling system should automatically track patterns you'd never catch manually. Which provider combinations lead to smoothest operations? When do specific locations experience demand spikes? How far in advance do different patient populations schedule? This data feeds monthly planning sessions but doesn't dictate decisions.
AI-powered operational software can identify capacity crises days or weeks before they happen. By analyzing booking patterns, provider schedules, and historical data, these systems flag potential problems while you have time to address them. The system doesn't automatically reassign providers—it presents options for human review.
For example, the system might alert: "Based on current booking velocity, Thursday afternoon at South clinic will exceed capacity by approximately 6 appointments. Options:
-
Extend Dr. Kumar's hours (has done this 2x this month)
-
Shift Jennifer NP from North (would leave pediatric coverage gap)
-
Open overflow to telemedicine (3 providers have virtual slots available).
Maintain human oversight of these recommendations. The system doesn't know Dr. Kumar's daughter has a recital Thursday evening, or that North clinic is running a vaccine campaign needing pediatric expertise, or that half your Thursday patients are elderly and struggle with telemedicine.
However, AI automation excels at administrative burden of capacity planning. Instead of manually pulling appointment data from three systems, software aggregates everything into your planning dashboard. Rather than scrolling through individual provider calendars, you get unified views of capacity gaps and bottlenecks across locations.
Common failure modes and recovery patterns
Well-designed capacity planning systems fail in predictable ways. Understanding these helps you build resilience and recover quickly.
The Expertise Bottleneck
You schedule based on provider availability but forget specialized expertise. You have coverage at every location, but your only provider comfortable with adolescent mental health is booked solid for three weeks. Parents start using emergency rooms for outpatient issues.
Recovery requires expertise development plans. Rather than hiring another specialist, train two existing providers in adolescent mental health basics. They won't replace the specialist but can handle straightforward cases and triage complex ones.
The Documentation Debt Spiral
Providers consistently run behind on documentation, staying hours after clinical time to complete notes. You add more clinical hours to meet demand, creating more documentation burden, forcing providers to stay even later. Eventually someone makes serious documentation errors from exhaustion.
The fix isn't "work faster" or "document during visits." Build documentation time into capacity planning—for every 4 hours of clinical time, allocate 1 hour administrative time. You might see fewer patients, but you'll prevent burnout and errors costing far more than empty appointment slots.
The Float Pool Failure
You maintain per-diem providers for coverage, but when needed, they're unavailable or unfamiliar with current workflows. The per-diem PA you call hasn't worked in six months and spends two hours figuring out your new EMR while patients wait.
Successful float pools require regular engagement. Schedule each per-diem provider for at least one monthly shift, even when not strictly needed. This maintains operational familiarity and practice connection. The cost of "unnecessary" shifts is nothing compared to competent coverage during crisis.
Building systematic resilience over perfect efficiency
The ultimate goal isn't perfect efficiency—it's systematic resilience maintaining quality care despite inevitable disruptions. This means building buffers, redundancies, and flexibility rather than optimizing for maximum utilization.
Target around 85% capacity utilization, not 100%. That buffer handles the unexpected—the sick provider, the flu outbreak doubling urgent care demand, the new insurance contract bringing 200 new patients. You're leaving money on the table by not booking every slot, but you're preventing much larger costs of cascade failures, provider burnout, and patient dissatisfaction when systems break under stress.
Target around 85% capacity utilization, not 100%. That buffer handles the unexpected—the sick provider, the flu outbreak doubling urgent care demand, the new insurance contract bringing 200 new patients. You're leaving money on the table by not booking every slot, but you're preventing much larger costs of cascade failures, provider burnout, and patient dissatisfaction when systems break under stress.
Ready to transform your practice workflow?
Join 2,000+ healthcare providers using GoCliny to increase efficiency, improve patient satisfaction, and grow revenue.