Mixed-visit practices lose shocking amounts to charge capture gaps. A cardiology group I worked with discovered they'd missed billing for EKG interpretations during telehealth follow-ups for six straight months — roughly $47,000 gone. The worst part? Their providers documented everything correctly. The breakdown happened between the provider finishing documentation and the coder pulling charges.
The charge capture checklist for mixed visits isn't about catching obvious mistakes. It's about systematically preventing the subtle misses that happen when your practice runs telehealth pre-screens, in-person consults, and same-day procedures across multiple providers and locations.
Why traditional charge capture fails with mixed modalities
Most practices built their charge capture around single-visit types. Your EMR prompts work fine for standard office visits. But throw in a telehealth consult that converts to an in-person procedure, and your billing team misses the transition codes, the facility fees, or the modifier adjustments.
The complexity multiplies when you consider how charges flow through your practice. A provider documents in the EMR during or immediately after the visit. Hours or days later, a coder reviews that documentation. Then billing staff enter charges. Each handoff creates an opportunity for missed charges, especially when visit types blend together.
Mixed-modality practices face unique charge capture challenges that single-format clinics never see. Your telehealth platform might not talk to your practice management system. Your providers switch between documentation templates depending on visit type. Your coders work from different charge sheets for virtual versus in-person encounters.
The real cost of charge capture failures
Beyond the obvious revenue loss, missed charges create cascading operational problems. Your billing team spends hours hunting for missing documentation. Providers get pulled into charge reconciliation meetings instead of seeing patients. Your days in AR climb because incomplete claims sit in work queues.
Eliminate appointment gaps and no-shows.
GoCliny streamlines every patient interaction from booking to billing—seamlessly.
- Unified appointment scheduling
- Automated patient reminders
- Staff calendar & task management
No credit card required
I analyzed charge capture data from 23 multi-specialty practices running hybrid models. The patterns were consistent: orthopedic practices missed injection codes during telehealth follow-ups, primary care missed transitional care management codes when mixing visit types, and specialty practices forgot facility fees for procedures scheduled from virtual consults.
The financial impact varies by specialty and volume, but practices typically lose 2-4% of potential revenue to charge capture gaps. For a practice seeing 400 patients weekly across mixed modalities, that translates to $35k-70k annually in missed charges.
Building visit-specific capture checklists
You need operationally distinct checklists for each visit modality that account for the specific charge risks of that format.
Telehealth Visit Charge Checklist
-
Verify patient location documented (affects billing jurisdiction)
-
Confirm audio-video versus audio-only modifier
-
Check for concurrent services (remote monitoring, care coordination)
-
Document technology platform used
-
Capture provider location if different from normal
-
Review for consultation codes if initiated by another provider
-
Flag for potential follow-up codes (TCM, CCM eligibility)
In-Person Consult Charge Checklist
-
Verify new versus established patient status
-
Document referral source for consultation billing
-
Capture all point-of-care testing performed
-
Check for injection/procedure codes beyond E&M
-
Review for preventive services during problem visits
-
Document teaching/counseling time if >50% of visit
-
Verify location of service matches POS code
Procedure Visit Charge Checklist
-
Confirm consent documentation for procedure billing
-
Capture all supplies and medications used
-
Document bilateral procedures with appropriate modifiers
-
Check for facility versus non-facility billing
-
Review for multiple procedures requiring modifier sequencing
-
Verify anesthesia type and provider if applicable
-
Document any complications affecting coding
These checklists work because they focus on the charges most commonly missed for each visit type, not generic reminders that apply to everything.
Common miss points by specialty
Different specialties have predictable charge capture blind spots based on their workflows and visit patterns.
Primary Care Mixed Visits
Primary care practices running both telehealth and in-person visits consistently miss transitional care management codes. A patient discharges from the hospital, has a telehealth follow-up within 48 hours, then an in-person visit the next week. The practice bills the individual visits but misses the TCM code worth an additional $130-190.
Annual wellness visits create another gap. When a patient schedules their Medicare wellness visit but also has acute concerns, practices often bill only the problem-focused E&M, missing the wellness visit that can be billed simultaneously with modifier 25.
Specialty Consults Across Modalities
Specialists lose charges when initial consultations happen via telehealth then convert to procedures. A dermatologist conducts a virtual consultation for a suspicious lesion, schedules an in-person biopsy two days later, but only bills the procedure — missing the consultation code entirely because it happened virtually.
Orthopedic practices face similar issues with injection visits. The provider documents the injection but forgets to capture the medication units, the bilateral modifier for joint injections, or the image guidance code when ultrasound is used.
Mental Health Hybrid Models
Psychiatric practices mixing telehealth and in-person visits frequently miss the complexity of medication management visits. They bill the standard 99213 or 99214 but don't capture the add-on psychotherapy codes when counseling extends beyond medication discussion. This oversight costs practices $40-65 per applicable visit.
Designing your coder handoff process
The gap between provider documentation and coder review creates most charge capture failures. Providers document what happened clinically. Coders translate that into billable charges. When these groups don't communicate effectively, charges disappear.
An orthopedic group I worked with solved this by implementing a 24-hour handoff protocol. Providers flag complex visits requiring coder review using specific EMR markers. Coders review flagged charts within one business day and send clarification requests back through the EMR task system. This simple process recovered $8,300 monthly in previously missed charges.
Your handoff process needs clear ownership and timeframes:
| Step | Responsibility | Timeframe |
|---|---|---|
| Provider completes documentation | Clinical team | During/immediately after visit |
| Chart routes to coding queue | System automation | Real-time |
| Coder reviews with modality checklist | Coding team | 24-48 hours |
| Questions route back to provider | EMR task system | Same day |
| Final charges post to billing | Billing team | 24 hours after coding |
Making this process systematic rather than relying on individual diligence prevents charges from slipping through. When every chart follows the same path with the same checkpoints, fewer charges disappear.
A simple workflow for the coder handoff looks like this.
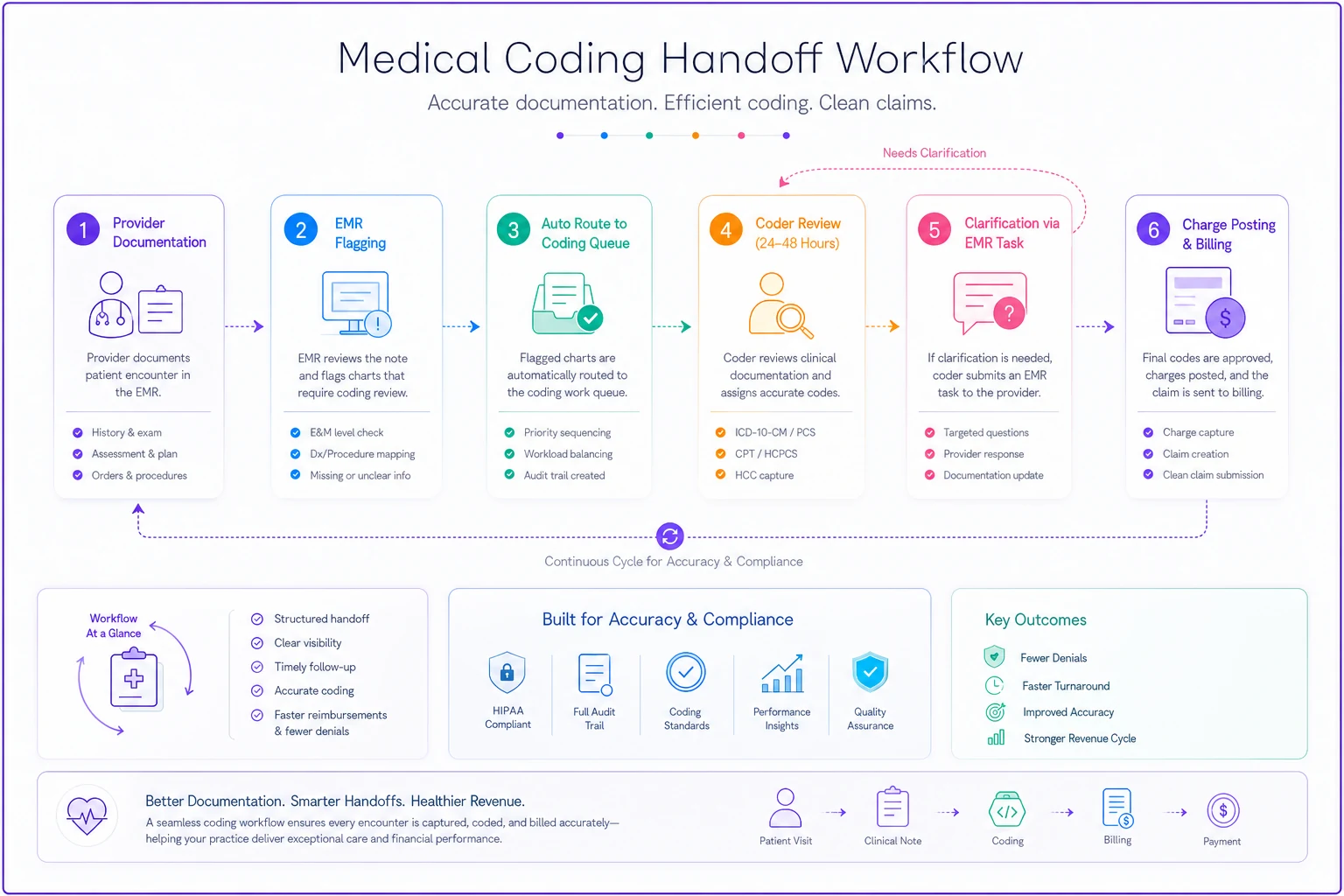
Use EMR flags to route complex charts to the coding queue automatically.
This handoff process needs ownership and timeframes to work reliably.
Post-session QA sampling that actually works
Random audits waste time and miss patterns. Effective QA sampling targets high-risk scenarios where charges commonly go missing.
Focus your QA efforts on:
-
Visits that convert from telehealth to in-person within 7 days
-
Procedures scheduled from virtual consultations
-
Visits with multiple providers or services
-
New patient visits via telehealth
-
Visits with time-based billing components
A multi-specialty group implemented targeted sampling of just 5% of visits — but specifically these high-risk categories. They found charge capture errors in 18% of sampled visits, compared to 3% in their previous random audits. More importantly, they identified systematic issues like consistently missing facility fees for minor procedures.
Your QA process should run weekly, not monthly. Weekly reviews catch patterns before they become expensive habits. Assign one person to pull the samples, another to review them, and a third to track patterns and update processes. This separation prevents any single person from becoming blind to recurring issues.
Quick fixes for common charge omissions
Most missed charges fall into predictable categories with straightforward fixes.
Missing Modifiers on Telehealth
Build modifier requirements into your EMR templates. When a provider selects telehealth as the visit type, the system should automatically prompt for audio-video versus audio-only documentation and apply the appropriate modifier. This single change can prevent hundreds of claim denials monthly.
Forgotten Injection Medications
Create standing order sets that include both the injection administration and the medication units. A trigger in your EMR can require medication documentation before allowing the provider to complete the injection procedure note.
Overlooked Facility Fees
Your scheduling system should flag when procedures move from office to facility settings. The scheduler confirms the location change with the billing team, who add facility billing to the encounter before the visit occurs.
Missed Time-Based Codes
Train providers to use EMR timers for visits where counseling might exceed 50%. The timer runs in the background, and if the threshold is met, the system prompts for time-based billing documentation.
Incomplete Preventive Services
Build Medicare wellness visit components into your rooming process. Medical assistants complete the required screenings and document them in discrete fields that automatically populate the wellness visit requirements.
Scenarios where charge capture breaks down
Real charge capture failures happen in predictable scenarios. Understanding these patterns helps you prevent them systematically.
The Converted Virtual Consult
A rheumatologist conducts a telehealth consultation for joint pain. During the visit, inflammation appears worse than expected. The provider schedules an in-person joint injection for the next day.
The charge capture breakdown: The practice bills the injection but misses the consultation code from the telehealth visit. They also forget to bill for the medication units and miss the bilateral modifier since both knees were injected. Total missed charges: $340.
The fix: Create linked encounter types in your EMR. When a telehealth visit generates a follow-up procedure within 72 hours, both encounters link automatically, prompting coders to review both for complete charge capture.
The Complex Chronic Care Patient
A primary care practice manages a diabetic patient through monthly telehealth check-ins with quarterly in-person visits for labs and foot exams. The provider spends 22 minutes on care coordination between visits.
The charge capture breakdown: The practice bills the individual visits but never captures chronic care management codes worth $42-84 monthly. Over a year, that's $500-1,000 in missed revenue per patient.
The fix: Build CCM tracking into your EMR workflows. When patients meet criteria (2+ chronic conditions), the system tracks all time spent on care coordination and automatically generates CCM charges when time thresholds are met.
The Multi-Provider Procedure Day
An urgent care schedules a patient for laceration repair. The physician evaluates and repairs the wound while a nurse administers a tetanus shot and applies a complex dressing.
The charge capture breakdown: The physician bills the E&M and repair. The injection and complex dressing codes never make it to billing because the nurse's documentation sits in a different section of the chart. Missed charges: $85.
The fix: Create encounter summaries that aggregate all services regardless of documenting provider. Your daily checklist for hybrid clinic days should include reviewing multi-provider encounters before charge submission.
Building your charge capture system
Effective charge capture isn't about perfect documentation or complex auditing. It's about building systematic checkpoints that catch common misses before claims go out.
Start with visit-specific checklists that address the actual risks of each modality. Don't create generic lists that providers ignore. Focus on the 5-7 items most commonly missed for each visit type.
Establish clear handoffs between providers and coders. Every chart needs a defined path from documentation to billing with specific timeframes and escalation procedures. This prevents charts from sitting in limbo while charges age past timely filing limits.
Then implement targeted QA sampling of high-risk scenarios. Don't waste time auditing routine visits that rarely have errors. Focus your limited QA resources on the conversions, complex visits, and multi-provider encounters where charges actually go missing.
Practices that capture charges successfully treat it as an operational system, not a documentation problem. They build the pre-submission QC workflows that catch errors systematically rather than relying on individual vigilance.
Modern practice management platforms can automate much of this charge capture workflow. AI-powered operational software can flag potential missed charges based on documentation patterns, route charts automatically based on complexity, and track handoff timing to prevent delays. Instead of manually checking every encounter against a checklist, your team focuses on the exceptions and patterns that need human judgment.
The bottom line on mixed-visit charge capture
Your charge capture problems aren't caused by lazy providers or incompetent coders. They're systematic gaps that emerge when practices run multiple visit modalities without modality-specific processes.
You need operational systems that account for the unique charge capture risks of telehealth, in-person, and procedure visits. Build distinct checklists for each modality. Create clear handoff protocols between documentation and coding. Focus QA efforts on high-risk scenarios rather than random sampling.
Stop treating charge capture as a back-office billing function. It's an operational process that starts the moment a patient schedules and doesn't end until the claim pays. Every person touching that patient encounter affects whether charges get captured correctly.
The practices recovering tens of thousands in missed charges aren't doing anything revolutionary. They're just building systematic processes that prevent predictable misses. They recognize that charge capture for mixed visits requires different operational workflows than single-modality practices.
Your providers want to capture charges correctly — they just need systems that make it automatic rather than requiring perfect memory and documentation. Give them visit-specific checklists, clear handoff processes, and targeted QA that catches patterns before they become expensive habits. The investment in building these systems pays for itself within weeks through recovered charges you're currently missing.
Stop treating charge capture as a back-office billing function. It's an operational process that starts the moment a patient schedules and doesn't end until the claim pays. Every person touching that patient encounter affects whether charges get captured correctly.
Ready to transform your practice workflow?
Join 2,000+ healthcare providers using GoCliny to increase efficiency, improve patient satisfaction, and grow revenue.