
Running mixed telehealth and in-person schedules feels like conducting two orchestras simultaneously. One provider's running 20 minutes late on a virtual visit while another needs the exam room they're using as their telehealth station. The front desk doesn't know whether to call the next patient in or keep them waiting. Someone inevitably knocks on the door mid-video call because they assumed the room was empty.
This isn't about sophisticated technology or complex systems—it's about basic operational reality. Most practices discovered the hard way that hybrid schedules break traditional clinic workflows in ways nobody saw coming.
Traditional clinic operations crumble with mixed visits
Traditional medical practices relied on physical proximity. Providers walked from room to room. Medical assistants knew where everyone was because they could see them. The front desk managed flow by watching the waiting room. Simple visual cues kept everything synchronized.
Add telehealth to that same day, and those visual cues vanish. The provider doing a virtual visit from exam room 3 looks "available" to anyone walking by. The front desk can't tell if a telehealth appointment is wrapping up or running long. Medical assistants prepare rooms for patients who might be sitting in their cars for a virtual visit instead of the waiting room.
Transitions create the biggest headaches. A provider finishing a complex in-person visit needs to switch mental gears, log into the telehealth platform, adjust their camera setup, and pull up the next patient's information—while the virtual patient sits in a digital waiting room wondering if they've been forgotten. That transition consistently takes 8-12 minutes when practices assume it takes 2.
One delayed transition creates a domino effect
A single botched transition costs more than most practices calculate. A dermatology practice in Austin tracks their hybrid days religiously. When a provider runs 15 minutes over on an in-person appointment, then needs to switch to telehealth, the delay compounds. The virtual patient, who blocked off exactly 30 minutes during their lunch break, drops off after waiting 18 minutes. The practice calls them back, plays phone tag for two days, and eventually squeezes them into an already packed schedule the following week.
Eliminate appointment gaps and no-shows.
GoCliny streamlines every patient interaction from booking to billing—seamlessly.
- Unified appointment scheduling
- Automated patient reminders
- Staff calendar & task management
No credit card required
-
A no-show that technically wasn't
-
Two days of staff time playing phone tag
-
An overbooked slot the following week
-
A frustrated patient who tells three coworkers that "telehealth doesn't really work"
-
Around $180 in direct lost revenue plus the harder-to-measure reputation damage
The front desk, trying to help, starts making executive decisions. They move the next in-person patient into a different room. But that room wasn't stocked for that type of visit. Now the medical assistant is running between rooms looking for supplies while the provider wonders why their patient isn't ready.
Building transition buffers that make sense
Successful hybrid practices build "transition buffers"—but not how you'd expect. Adding 10 minutes between every appointment sounds logical until you realize that's potentially 80 minutes of lost revenue per provider per day.
Practices that run smooth hybrid schedules create dynamic buffers instead. After any in-person appointment requiring room turnover (procedures, complex exams), they schedule telehealth visits specifically because the provider can start those from anywhere. After back-to-back telehealth appointments, they schedule simple follow-ups in-person that don't require extensive room prep.
-
In-person to telehealth
5 minutes (provider can start from current location)
-
Telehealth to in-person
8 minutes (includes walking to room, washing hands, reviewing chart)
-
Complex procedure to anything
12 minutes (room turnover plus provider reset)
-
Back-to-back telehealth
2 minutes (just close and reopen platform)
These aren't rigid rules. A family medicine practice in Denver adjusts buffers based on the provider. Dr. Martinez, who's been doing telehealth for three years, needs 3 minutes between virtual visits. Dr. Chen, who still occasionally forgets to unmute herself, gets 5 minutes.
The numbers work out better than expected. Instead of adding blanket time between all appointments, strategic buffers only affect certain transition types.
Tech checks that catch the real problems
Every practice claims they do tech checks. Most do them wrong. Running a test call the day before doesn't catch the problems that kill hybrid schedules.
The tech check that matters happens 90 minutes before the first telehealth appointment of the day. Not the night before, not first thing in the morning—90 minutes before. This timing catches morning update issues, network slowdowns from everyone logging in, and gives enough time to actually fix problems.
-
73% of tech failures happen with the first telehealth appointment of the day
-
Morning operating system updates cause about 30% of platform crashes
-
Audio issues outnumber video issues 4 to 1
-
The provider's connection fails more often than the patient's
Their tech check routine now includes having someone from the front desk join a test call from the patient's perspective. Takes four minutes, catches issues like the provider's microphone defaulting to the computer instead of their headset, or the exam room's WiFi extender being unplugged by the cleaning crew.
Have the front desk test from the patient's device type (phone vs. computer) to catch platform-specific link issues.
This timing and routine turns a once-a-week ritual into a meaningful safeguard that actually prevents the morning meltdown.
Front desk scripts that handle complex handoffs
The front desk becomes air traffic control on hybrid days. They need different scripts for different scenarios, and generic templates don't work.
"Dr. Johnson is finishing up with another patient. I'll let you know as soon as the room is ready—should be about 10 minutes. Would you like to wait here or in your car? I can text you when we're ready."
"I see you're scheduled for video visit. Are you using a computer or phone? Okay, on your phone—do you see the link we texted you this morning? Click that and it should open... still not working? No problem, Dr. Smith can switch to a phone visit. She'll call you at this number in about 3 minutes."
"Dr. Anderson is wrapping up an appointment. We're running about 8 minutes behind. You're welcome to wait, or if you'd prefer, there's a coffee shop next door—I can text you when we're ready."
The scripts seem basic, but they prevent the front desk from overpromising ("just a few more minutes" when it's actually 20) or creating confusion ("the doctor will see you soon" when the patient doesn't know if that means 2 minutes or 30).
Handoff rules that prevent coordination failures
The handoff between front desk, medical assistants, and providers breaks down predictably on hybrid days. A medical assistant prepares a room for an in-person patient, not realizing the provider switched the order to handle an urgent telehealth follow-up first. The front desk tells a patient their telehealth appointment is starting, but the provider is still documenting the previous visit.
Clear handoff rules prevent about 80% of these coordination failures.
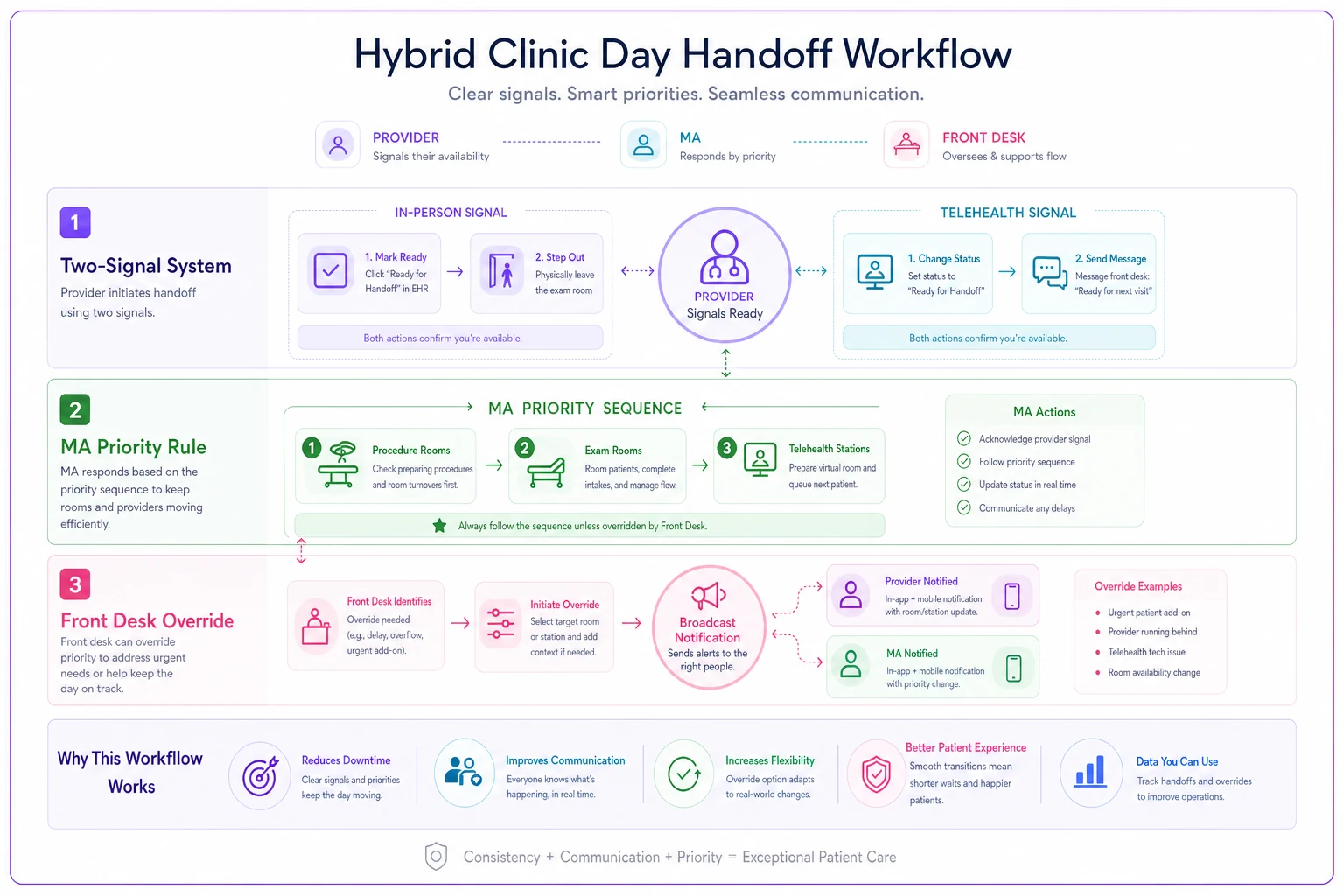
The Two-Signal System: Providers signal readiness two different ways. For in-person: they mark themselves "ready" in the scheduling system AND physically step out of the room. For telehealth: they change their status AND send a quick message to the front desk. Redundancy prevents the "I thought you were ready" confusion.
The MA Priority Rule: Medical assistants prioritize room prep based on visit type, not appointment time. Procedure rooms first (longest turnover), then standard exam rooms, then telehealth stations. This prevents the 2:30 procedure from starting late because the MA was setting up a basic follow-up room.
The Front Desk Override: Front desk staff can override the schedule order if they see a better flow. Virtual patient ready early while in-person is running late? Switch them. But they must notify both the provider and MA immediately through the practice's communication system, not verbal handoffs that get forgotten.
The workflow below shows how the Two-Signal System, MA Priority Rule, and Front Desk Override interact during hybrid day handoffs.
Most practices underestimate how much coordination happens through visual cues. When providers are scattered between physical rooms and virtual calls, those visual cues disappear.
Actual schedules from practices making hybrid work
A pediatric practice outside Portland shares their actual Tuesday schedule to show how this works. They see roughly 45 patients on hybrid days, with about 40% being telehealth.
| Time | Appointment Type | Duration | Visit Mode | Notes |
|---|---|---|---|---|
| 8:00 | New patient physical | 30 min | In-person | Buffer telehealth after |
| 8:30 | ADHD follow-up | 15 min | Telehealth | Natural transition time |
| 8:45 | Well child check | 20 min | In-person | Quick room turnover |
| 9:05 | Parent consultation | 15 min | Telehealth | Provider can start anywhere |
| 9:20 | Sick visit | 15 min | In-person | Similar visit types |
| 9:35 | Sick visit | 15 min | In-person | Back-to-back efficiency |
| 9:50 | Mental health check | 20 min | Telehealth | Gives MA catch-up time |
| 10:15 | Admin buffer | 5 min | - | Schedule flexibility |
| 10:20 | Telehealth follow-up | 15 min | Telehealth | Start of cluster |
| 10:35 | Telehealth follow-up | 15 min | Telehealth | Maintain momentum |
| 10:50 | Telehealth follow-up | 15 min | Telehealth | End cluster strong |
Notice the pattern: they cluster telehealth visits after potentially complex in-person appointments. The ADHD follow-up after a new patient physical gives buffer if the physical runs long. The mental health check after two sick visits provides natural transition time. The three consecutive telehealths at the end lets the MAs catch up on room prep for the afternoon.
Afternoon scheduling shows a different strategy. They front-load in-person visits from 1:00 - 3:00 when families are doing school pickups, then shift heavily to telehealth from 3:00 - 5:00 when parents can step away from work for a video call.
The practice tested several approaches before settling on this pattern. Random mixing of in-person and telehealth appointments created chaos. Alternating strictly between modes felt forced and created unnecessary transitions.
When hybrid scheduling backfires
Some practices shouldn't run hybrid schedules. A plastic surgery clinic tried mixing virtual consultations with in-person procedures. The constant switching between detailed physical examinations and screen-based discussions destroyed their efficiency. They lost around $12,000 in monthly revenue before admitting defeat.
-
Providers can't maintain focus while switching contexts
-
The practice lacks dedicated telehealth spaces
-
Visit types require completely different mindsets or equipment
-
The front desk is already overwhelmed with basic operations
A better approach for these practices: dedicated telehealth blocks or days rather than mixing visit types. One orthopedic group runs telehealth only on Tuesday afternoons and Thursday mornings. No transitions, no confusion, predictable workflow.
The decision often comes down to provider temperament. Some doctors thrive on variety and context-switching. Others get mentally exhausted jumping between physical exams and video calls all day.
Tracking whether your hybrid operations actually work
Monitor three specific metrics to know if your hybrid scheduling checklist helps:
Transition delays: Time between scheduled appointment end and when the next appointment actually starts. Should average under 5 minutes for same-type visits, under 8 minutes for transition visits. Anything over 10 minutes consistently means your buffers aren't working.
Ghost no-shows: Patients marked as no-shows who were actually waiting (in the virtual waiting room, in their car, in the wrong physical waiting area). More than 2-3 per week indicates handoff problems.
Daily completion rate: Percentage of scheduled appointments actually completed (not rescheduled, not converted from video to phone). Healthy hybrid practices maintain 92% or higher. Below 85% means operational chaos.
These metrics tell you more than revenue numbers because they catch problems before they become financial losses.
Managing the permanent complexity of mixed modalities
Hybrid schedules aren't temporarily complicated—they're permanently complex. Practices that succeed with mixed telehealth and in-person visits accept this complexity and build operations around it. They don't try to force virtual visits into physical visit workflows.
The checklist and protocols matter, but the mindset shift matters more. Your front desk isn't just checking patients in—they're coordinating two parallel operations. Your medical assistants aren't just prepping rooms—they're managing both physical and digital patient flow. Your providers aren't just seeing patients—they're constantly switching between two different modes of care delivery.
Some practices discover that AI-powered scheduling and coordination software removes about 70% of the manual coordination burden. The software tracks transition times, automatically adjusts buffers based on actual performance, and alerts staff to potential conflicts before they cascade. Even with intelligent automation handling the complex orchestration, the fundamental challenge remains: hybrid schedules require different operational thinking.
Practices succeeding with hybrid schedules didn't get there by adding more rules or buying better telehealth platforms. They recognized that mixed modalities create new operational patterns, then built their daily operations around those patterns instead of fighting them.
Your hybrid visit scheduling checklist shouldn't be a band-aid on broken workflows. It should be the foundation of an entirely different operational approach—one that assumes complexity, plans for transitions, and gives your team the tools and protocols to manage two different types of care delivery at the same time.
Ready to transform your practice workflow?
Join 2,000+ healthcare providers using GoCliny to increase efficiency, improve patient satisfaction, and grow revenue.