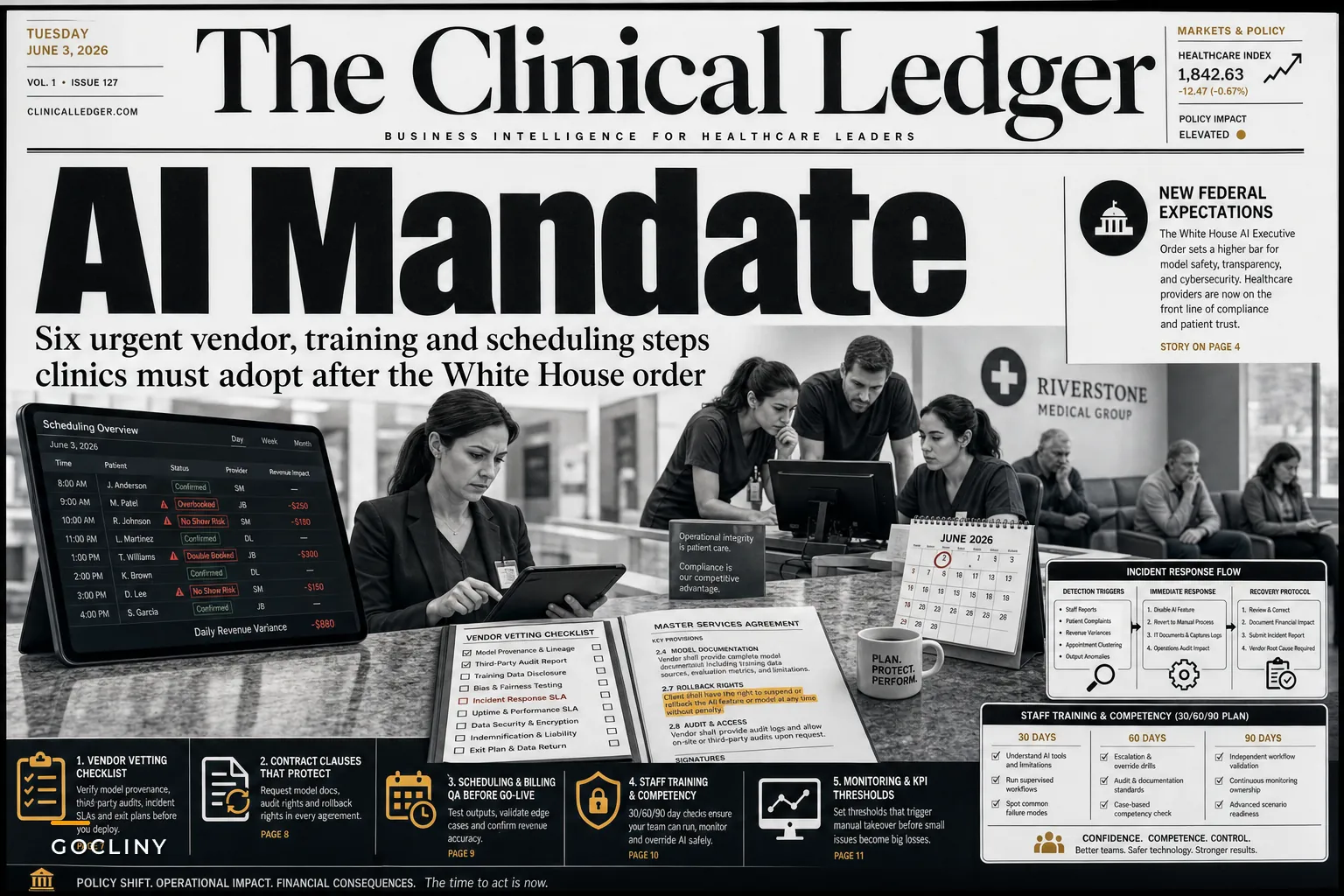

Yesterday's White House executive order on AI dropped a compliance problem squarely on healthcare practices. The order asks AI developers to submit models for voluntary government review while establishing new expectations around safety, provenance, and cybersecurity. Practically speaking: that scheduling assistant your EMR vendor just rolled out, the automated prior-auth tool you're testing—every AI feature touching patient data now sits in potential federal crosshairs.
Most clinic managers I talk to barely finished their HIPAA updates from last year. Now they're getting vendor emails about "AI transparency commitments" and "model provenance documentation" without really knowing what questions to ask or which contract clauses actually matter.
The real operational problem isn't the executive order itself. It's that your current vendor agreements probably don't address AI incident response, your staff training doesn't cover AI output verification, and your billing team has no protocol for when automated coding suggestions go wrong.
The vendor vetting gap nobody's talking about
Three weeks ago, a 12-provider orthopedic clinic in Phoenix found out their new AI scheduling optimizer had been quietly trained on data from other practices. Not a HIPAA breach exactly, but the vendor couldn't explain why the system kept suggesting appointment patterns that matched a competing clinic's workflow. The practice manager spent around 40 hours auditing three months of schedules and found roughly $18,000 in lost revenue from bad booking patterns.
This is happening in a lot of places. Practices pick up AI features through routine software updates without any real vetting process. Your EMR adds "intelligent scheduling suggestions." Your billing platform launches "automated denial predictions." Your patient portal gets "smart appointment reminders." Each one shows up as a checkbox in your settings panel with zero documentation about the underlying model, training data, or what happens when it fails.
The executive order changes this. Vendors will eventually need to provide model documentation, safety testing results, and incident response plans. But what matters for your operations right now is that you need to update your vendor contracts and evaluation criteria before your next renewal cycle—not after vendors figure out their own compliance story.
Step 1: Audit your current AI exposure across all systems
Pull every vendor contract from the last 18 months. Look for any mention of:
Eliminate appointment gaps and no-shows.
GoCliny streamlines every patient interaction from booking to billing—seamlessly.
- Unified appointment scheduling
- Automated patient reminders
- Staff calendar & task management
No credit card required
-
Machine learning
-
Predictive analytics
-
Automated decision-making
-
Intelligent features
-
Smart recommendations
A typical 8-provider primary care practice runs around 14 different software systems. Based on what we see across practices, at least 9 of those now include some AI component—usually added through updates without any explicit notification.
Build a simple tracking sheet:
| System | AI Features | Data Used | Vendor Documentation | Risk Level |
|---|---|---|---|---|
| EMR | Coding suggestions | Patient encounters | None provided | High |
| Scheduler | Optimization | Appointment history | Marketing sheet only | Medium |
| Billing platform | Denial prediction | Claims data | Technical overview | Medium |
| Patient portal | Response automation | Message history | None | High |
Anything without clear documentation gets flagged as high risk. Those are your first vendor conversations.
Step 2: Demand model transparency before, not after, adoption
Vague "our AI improves outcomes" claims aren't good enough anymore. Every vendor conversation now needs specific technical answers:
Training data sources: Where did the data come from? Other healthcare organizations? Public datasets? Synthetic data? A cardiology practice in Miami found their telemedicine platform's triage AI was trained mostly on emergency department data—completely wrong for routine virtual visits.
Update frequency: How often does the model retrain, and on whose data? One pediatric clinic found their appointment reminder AI got progressively worse over six months because it was retraining on aggregate data dominated by adult practices.
Failure modes: What happens when the AI fails? A dermatology group discovered their automated referral system had no fallback when confidence scores dropped below threshold—it just stopped processing referrals for two days without alerting anyone.
Audit capabilities: Can you review AI decisions after the fact? Most platforms offer zero visibility into why their AI made specific recommendations. You need logs showing inputs, confidence scores, and decision paths.
Step 3: Build staff verification protocols for every AI touchpoint
Your front desk uses AI-suggested appointment slots. Your billers review AI-generated coding recommendations. Your nurses see AI-prioritized message queues. Each of those interactions needs a verification step—not because AI always fails, but because when it does, the damage compounds fast.
Here's what verification looks like in practice:
Scheduling verification: When the system flags an unusual booking pattern, staff checks it against standard protocols. One family practice noticed their AI consistently suggested 15-minute slots for complex cases because it was optimizing for volume, not clinical appropriateness.
Billing verification: Every AI-suggested code gets human review for medical necessity and documentation support. An orthopedic clinic caught their AI consistently upcoding injection procedures based on supply costs rather than services actually rendered.
Communication verification: Automated patient responses get spot-checked daily. An urgent care chain found their chat AI had been giving outdated vaccine information for three weeks after CDC guidelines changed.
Place quick verification checkpoints at natural handoffs (when schedules print, when bills batch, when message queues refresh) to catch AI errors early.
The verification doesn't have to slow things down. Design it as quick checks at natural handoff points—when schedules print for the day, when bills batch for submission, when message queues refresh.
Step 4: Document AI-specific incident response procedures
When your scheduling AI crashes, who decides to switch to manual booking? When billing AI flags clearly wrong codes, who reviews the last week of submissions? When patient communication AI sends something it shouldn't, who handles the fallout?
Most practices have downtime procedures for system failures but nothing specific to AI malfunctions. That gap matters because AI failures are often partial and hidden. The system keeps running—just badly.
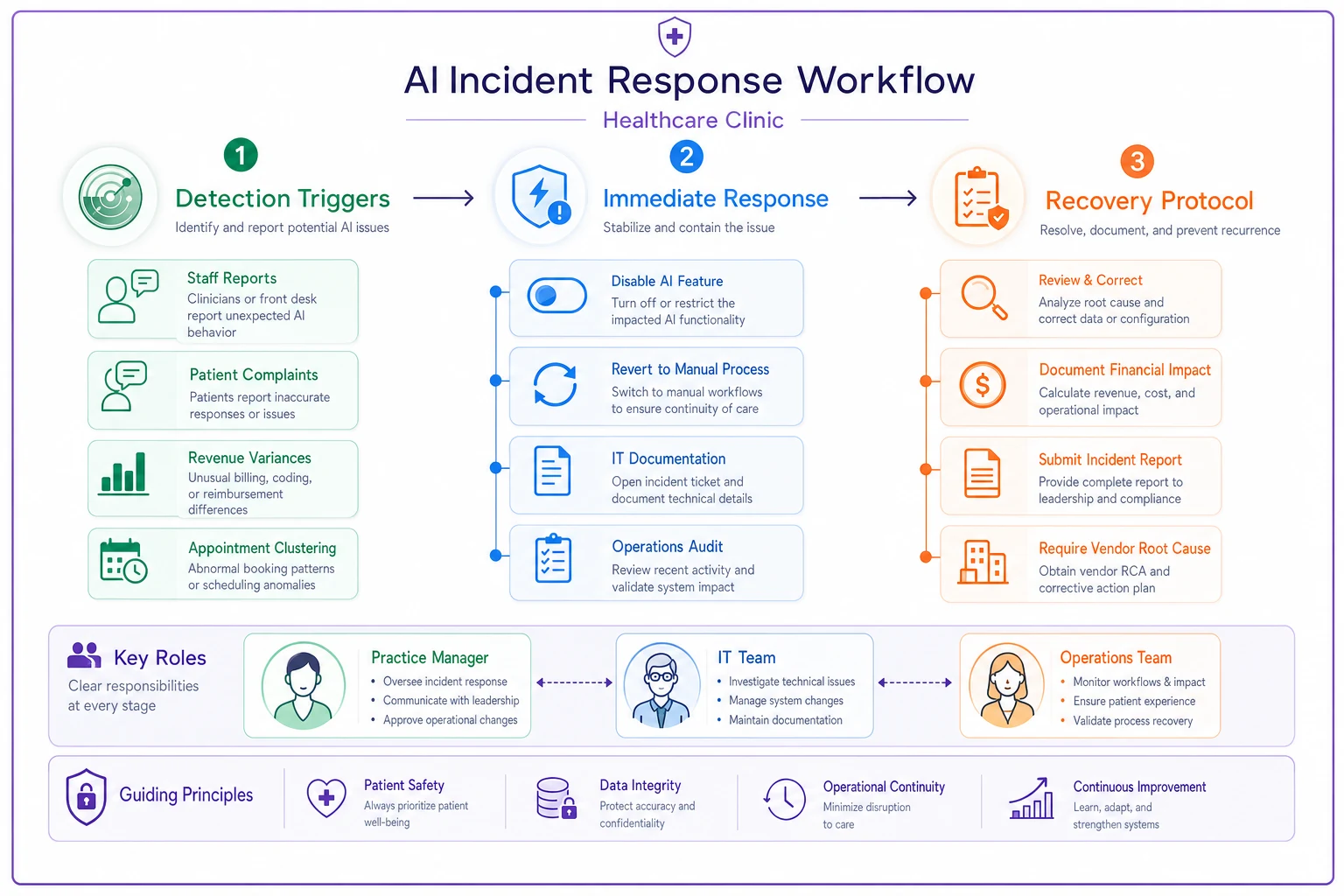
A multi-location pediatric group built this response matrix after their appointment AI started clustering all well-child visits on Mondays:
-
Staff reports unusual patterns
-
Patient complaints about scheduling
-
Revenue variances over 8%
-
Appointment type clustering exceeding 40%
Immediate response:
-
Designated manager disables the AI feature
-
Team reverts to manual process
-
IT documents current AI settings
-
Operations lead audits the last 48 hours of AI decisions
Recovery protocol:
-
Review and correct affected schedules, bills, or communications
-
Document financial impact
-
Submit incident report to vendor
-
Require vendor root cause analysis before reactivation
This diagram shows the flow from detection to recovery in a simple, operational way.
According to Reuters coverage of the order, the federal review process will likely require vendors to maintain similar incident documentation. Getting ahead of that requirement protects your operations and gives you real leverage in vendor negotiations.
Step 5: Add AI competency to your training matrix
Your existing staff onboarding system with competency checkpoints needs AI-specific modules at each milestone. New hires need to understand not just how to use AI features, but when to override them.
30-day AI competencies:
-
Identify which workflows include AI assistance
-
Recognize obvious AI errors
-
Know escalation procedures for AI issues
-
Understand manual fallback processes
60-day AI competencies:
-
Verify AI recommendations against protocols
-
Document AI-related issues properly
-
Train others on AI verification steps
-
Spot patterns in AI failures
90-day AI competencies:
-
Audit AI performance in their area
-
Suggest workflow improvements for AI integration
-
Lead AI incident response for their function
-
Maintain AI feature documentation
A 6-location primary care network found that adding explicit AI training cut AI-related errors by roughly 70% in the first quarter. More importantly, staff stopped blindly accepting AI suggestions and started treating them as inputs requiring their own professional judgment—which is exactly how it should work.
Step 6: Renegotiate contracts with AI-specific protections
Your next vendor renewal needs new contract language. Waiting for "industry standard" terms means operating without protection for months or longer.
Start with these non-negotiables:
Performance guarantees: AI features must hit specified accuracy levels. One urgent care chain requires 94% coding suggestion accuracy or automatic service credits kick in.
Transparency requirements: Vendors must provide model documentation, training data descriptions, and update notifications. A dermatology group requires 30-day advance notice of any model changes affecting clinical workflows.
Liability allocation: Clear assignment of responsibility for AI errors. Most vendor standard contracts disclaim all AI-related liability—that's completely unacceptable when AI is driving your revenue cycle or patient scheduling.
Audit rights: The ability to review AI decision logs, test model performance, and bring in third-party assessments if needed. A cardiology practice requires quarterly performance reports showing AI accuracy broken down by workflow type.
Termination triggers: The right to disable AI features or exit contracts if compliance requirements change. With federal AI regulation still evolving, you need exit ramps that don't destroy your operations.
What happens when practices ignore AI vendor vetting
A 15-provider multi-specialty clinic learned this the hard way. They adopted an "AI-powered" revenue cycle platform in January without proper vetting. The system promised a 23% improvement in clean claim rates through automated coding optimization.
By March, their denial rate had jumped from 8% to 14%. The AI was adding modifiers based on patterns from hospital billing—completely wrong for outpatient claims. Their billing team spent 200 hours fixing claims and resubmitting denials.
The vendor's response? The model was "working as designed" and would "improve over time with more data." The contract had no performance guarantees, no audit rights, and a three-year commitment with heavy early termination penalties.
They eventually negotiated an exit after documenting $127,000 in lost revenue and added labor costs. The replacement system—properly vetted this time—required detailed model documentation, monthly performance reports, and contractual accuracy guarantees.
Moving from reactive to proactive AI governance
The federal executive order signals something straightforward: AI in healthcare is no longer experimental. It's operational, it's being regulated, and it requires the same rigor as any other critical system in your practice.
Smart practices aren't waiting for final regulations. They're building AI governance into their operational framework now—updating vendor criteria, training staff properly, and creating safety nets for when AI inevitably fails.
The choice isn't whether to use AI in your practice. These features are already embedded in your current systems, arriving through updates and new releases whether you explicitly adopted them or not. The choice is whether you control how AI affects your operations or let vendors make those decisions for you.
Start with the six steps above. Audit your exposure. Demand transparency. Train your staff. Build response procedures. Update your contracts. Each step protects your practice from the hidden risks of ungoverned AI while putting you in a position to actually benefit from the features that work.
The practices doing well with AI aren't the ones with the most advanced features. They're the ones who treated AI vendor vetting as seriously as they treat HIPAA compliance—before regulators forced them to.
Ready to transform your practice workflow?
Join 2,000+ healthcare providers using GoCliny to increase efficiency, improve patient satisfaction, and grow revenue.