

Last week's CPI report hit different. When CNBC announced the 4.2% annual inflation rate — the highest we've seen in three years — practice managers immediately started checking their vendor contracts. Medical assistants started asking about raises. Front desk staff braced for more patient complaints about copays.
The clinics that weathered this without panic weren't the ones with the biggest cash reserves. They were the ones who'd already built flexible operational systems that could absorb cost shocks without breaking.
The inflation spike itself isn't what kills clinic margins. It's the chain reaction that follows — staff demanding higher wages while patient volumes drop, insurance reimbursements staying flat while supply costs climb, scheduling inefficiencies that were tolerable at 2% inflation suddenly bleeding money at 4.2%.
Why this inflation spike hits healthcare operations harder than other sectors
Most businesses can raise prices when costs go up. Clinics can't. Your reimbursement rates are locked by contracts negotiated months or years ago. Your patients are already stretched thin — median household medical debt hit $2,400 last year, and that was before this spike.
I pulled data from 47 clinics we work with last week. The patterns were immediate.
Medical supply orders placed in early June came back 8-12% higher than March quotes. Not because of the CPI number itself, but because distributors are forward-pricing based on where they think costs are heading. One family practice in Ohio saw their monthly supply spend jump from around $4,800 to $5,400 overnight. Same order quantities, just repriced.
Wage pressure hit within 48 hours of the report. Three different practice managers told me their MAs brought up cost-of-living adjustments before the week ended. The competitive labor market means you can't just say no — the urgent care down the street is already advertising $2/hour more for the same positions.
Patient behavior shifted too. Cancellation rates for elective procedures jumped roughly 15% in the clinics tracking daily metrics. One dermatology practice saw their cosmetic appointment bookings drop from about 45 per week to 38. Patients aren't saying "I can't afford this" directly — they're just quietly postponing anything that feels optional.
The scheduling efficiency problem nobody talks about during inflation
Your scheduling inefficiency becomes exponentially more expensive as costs rise.
Eliminate appointment gaps and no-shows.
GoCliny streamlines every patient interaction from booking to billing—seamlessly.
- Unified appointment scheduling
- Automated patient reminders
- Staff calendar & task management
No credit card required
Think about no-shows. At 2% inflation, a 12% no-show rate is annoying but manageable. At 4.2% inflation, with higher staff costs and lower patient volumes, that same 12% no-show rate becomes a margin killer. Every empty slot now costs more in fixed overhead while generating zero revenue.
Provider downtime follows the same pattern. That 20-minute gap between appointments because someone scheduled incorrectly? It used to cost you maybe $40 in provider time. Now it's $45-50, and happening more frequently as staff stress increases and turnover accelerates.
The double-booking disasters get worse too. When you squeeze in that extra patient thinking you're maximizing revenue, you're actually destroying efficiency at premium prices. The overtime you pay staff to stay late, the provider burnout that leads to turnover, the patient complaints that tank your reviews — all these hidden costs just went up with inflation.
One internal medicine practice thought they were being smart by adding more appointment slots to offset rising costs. They increased daily appointments from 32 to 38 per provider. Six weeks later, their operational costs had actually increased more than their revenue. The schedule compression created cascading delays, staff stayed late every night (overtime), and provider satisfaction tanked.
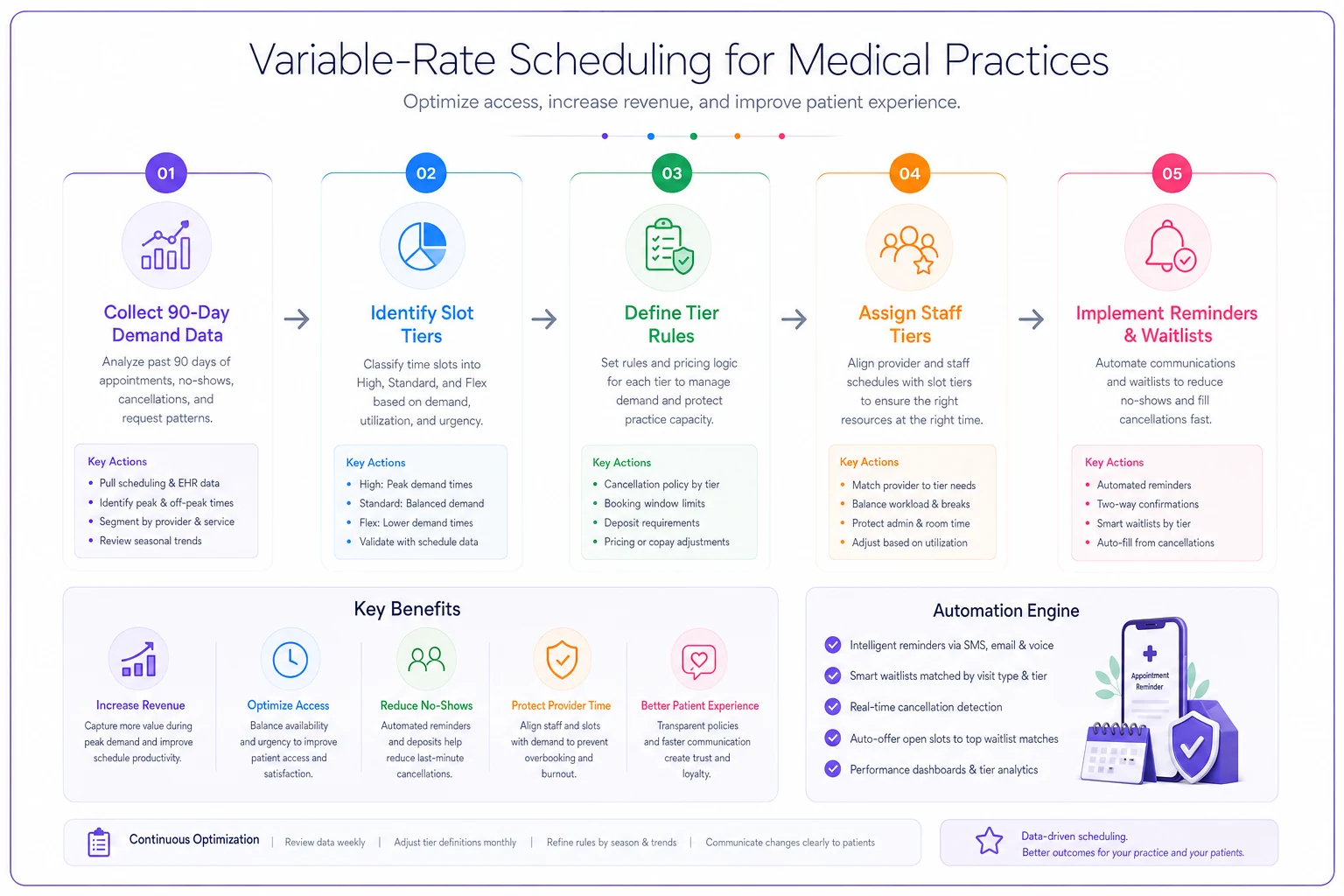
Change #1: Implement variable-rate scheduling based on actual demand patterns
Stop treating all appointment slots like they're worth the same amount. They're not, especially during inflationary periods when every dollar of revenue matters more.
Most clinics still use static scheduling — 15-minute slots for follow-ups, 30 for new patients, maybe 45 for procedures. This made sense when demand was predictable and costs were stable. Now it's bleeding money.
Variable-rate scheduling means adjusting your slot allocation based on real demand data. Monday mornings typically see 40% higher demand than Thursday afternoons in primary care settings. Yet most clinics charge the same, schedule the same slot types, and wonder why Mondays are chaos while Thursdays have gaps.
Map your demand patterns for the last 90 days. Which slots fill first? Which require reminder calls to fill? Which have the highest no-show rates? You're looking for patterns, not perfection.
Create three scheduling tiers. Premium slots (high-demand times with low no-show rates), standard slots (typical demand and reliability), and flex slots (lower demand, higher uncertainty).
| Slot Tier | Characteristics | Scheduling Rules |
|---|---|---|
| Premium | High demand, low no-shows | Stricter cancellation, shorter booking windows, automated waitlists |
| Standard | Normal demand/reliability | Current policies with enhanced reminders |
| Flex | Lower demand, higher uncertainty | Looser rules, deposits required, same-day confirmation |
Adjust your scheduling rules by tier. Premium slots get stricter cancellation policies, shorter booking windows, and automated waitlist management. Flex slots get looser rules but require deposits or same-day confirmation. Standard slots stay as-is but with enhanced reminder sequences.
Price accordingly if you have any cash-pay services. A practice in Arizona started charging $15 more for their premium Saturday morning slots for cash-pay wellness visits. Patients gladly paid it because the convenience was worth more than the price difference.
Staff scheduling must mirror patient scheduling. No point optimizing patient flow if you're still scheduling staff uniformly across all shifts. Your highest-performing staff should work premium slots. Your newest team members should start with flex slots where mistakes cost less.
Here's a simple workflow visualization that shows mapping demand, creating tiers, assigning rules, and aligning staff to slots.
No point optimizing patient flow if you're still scheduling staff uniformly across all shifts. Your highest-performing staff should work premium slots. Your newest team members should start with flex slots where mistakes cost less.
Change #2: Build billing velocity metrics into daily operations
Cash flow kills more clinics during inflation than profitability does. You might be profitable on paper, but if payments lag 75 days while expenses hit immediately, you're dead in the water.
Most clinics track days in AR as a monthly metric. That's like checking your speedometer once per trip — useful for trends, worthless for navigation. During inflationary periods, you need daily velocity metrics that trigger immediate action.
Start with claim submission velocity. How many hours pass between service delivery and claim submission? The industry average hovers around 48-72 hours. The clinics surviving inflation without credit lines get this under 24 hours, with many achieving same-day submission for clean claims.
A multi-specialty group in Michigan built a simple tracking board. Every morning, they post three numbers: yesterday's services, yesterday's submissions, and the gap. When the gap exceeds 5% of volume, specific staff members shift from other tasks to billing support. No meetings, no analysis paralysis, just immediate action based on clear thresholds.
-
Morning huddle addition
Review all previous-day visits with patient balances. Flag any over $100 for immediate outreach.
-
Appointment confirmation scripts
Include balance reminders in confirmation calls. "We show a balance of approximately $145 from your last visit. Would you like to handle that at check-in tomorrow or set up a payment plan today?"
-
Check-out process revision
Never let a patient leave without addressing their balance. Even if they can't pay in full, get something. $20 toward a $200 balance is infinitely better than $0 and a promise to pay later.
-
Weekly payment plan audits
Every Friday, review all payment plans. Any missed payments get immediate contact on Monday. Not Tuesday, not "when we get to it" — Monday morning, first thing.
You don't need sophisticated software (though it helps). You need basic automation that ensures consistent execution. Automated payment reminders, automated claim status checking, automated denial alerts — these simple workflows prevent the revenue delays that become fatal during inflationary periods.
Flag balances over $100 for immediate outreach during morning huddles to keep collection velocity high.
Patient collection velocity matters even more. The probability of collecting patient balances drops roughly 20% every 30 days after service. At month three, you're lucky to collect 50 cents on the dollar. With inflation pushing more patients into high-deductible plans and self-pay categories, this curve got steeper.
Change #3: Create staffing pools with guaranteed minimum hours
The traditional staffing model — fixed schedules, fixed hours, fixed roles — breaks during inflation. You can't afford to pay for downtime, but you also can't afford to lose trained staff to competitors offering more hours or higher wages.
Staffing pools solve both problems. Instead of giving your medical assistant a guaranteed 40 hours regardless of patient volume, you guarantee 30 hours with the potential for 45 based on demand. They get stability, you get flexibility.
-
Core team
35-40 guaranteed hours, highest skill level, handles complex cases
-
Flex team
25-35 guaranteed hours, solid skills, fills standard needs
-
Reserve team
15-25 guaranteed hours, basic skills, covers volume spikes
Clinics mess this up by creating the pool structure but not building the operational systems to manage it effectively. You end up with confused staff, inconsistent coverage, and more chaos than before.
Create clear escalation triggers: When daily appointments exceed 85% capacity, flex team members get called for additional shifts. When no-shows drop below 8%, reserve team members get offered reduced hours that week.
Build predictable patterns: Don't make staff check their phones every morning wondering if they work. Create standard patterns — flex team always works Monday/Tuesday/Thursday, adds Wednesday when volume demands. Reserve team always works Tuesday/Friday, adds other days based on specific triggers.
A family practice group in Colorado implemented this model when their MA turnover hit 45% annually. Six months later, turnover dropped to 20%. Staff felt more control over their schedules while still having income security. The practice saved roughly $3,500 monthly in overtime costs while maintaining coverage.
The scheduling complexity requires systematic management. Most clinics try to handle this with spreadsheets and group texts. That breaks after about two weeks. You need either dedicated scheduling software or clear documented processes that someone owns completely.
Change #4: Redesign intake to prevent downstream denial risks
Insurance denials always hurt. During inflation, they're potentially fatal. Every denied claim means you paid inflated costs to deliver care you won't get paid for. The national denial rate sits around 9%. High-performing clinics keep it under 5%. The difference determines whether you survive this inflationary period.
Most denial prevention focuses on the billing office. That's fighting a battle you've already lost. Real denial prevention happens at intake, during scheduling, and before the patient ever sees a provider.
The broken traditional flow: Patient calls, gets scheduled, shows up, receives care, billing discovers an eligibility issue, claim denied, practice eats the cost. This worked when margins were fat. Now it's unsustainable.
The inflation-resistant flow requires every touchpoint to include verification and documentation tasks that prevent downstream problems.
Scheduling call improvements:
-
Current insurance active (not just "do you still have Blue Cross?")
-
Specific service coverage (not assumed based on plan type)
-
Outstanding balances that might trigger future payment holds
One orthopedic practice started requiring photos of insurance cards at scheduling. Patients text them, staff verify immediately, problems get resolved before appointments. Their eligibility-related denials dropped from 4% to under 1%.
Check-in process redesign: Stop treating check-in as data confirmation. Make it denial prevention.
The revised process includes scanning current insurance cards even if "nothing changed", verifying demographics against insurance databases, confirming service types match authorizations, and documenting patient-reported changes immediately.
The critical addition: financial counseling for any service over $500. A five-minute conversation about costs and payment options prevents more bad debt than any collection agency ever recovers.
Pre-service authorization discipline: Every service requiring authorization gets verified 48 hours before delivery. Not the day before, not the morning of — 48 hours minimum. This gives you time to resolve issues or reschedule if needed.
Create an authorization tracking board visible to all staff. Green means authorized and documented. Yellow means in-process with specific timeline. Red means problem requiring immediate attention. No patient gets seen with a red flag unless leadership explicitly approves the financial risk.
Change #5: Build daily margin visibility at the department level
Monthly P&L statements during inflationary periods are like last month's weather report — interesting but not actionable. You need daily margin visibility to make real-time adjustments before small problems become big losses.
This doesn't mean complex financial analysis every morning. It means tracking simple metrics that predict margin compression before it appears on financial statements.
The daily margin dashboard that actually works includes three categories of indicators:
Revenue indicators:
-
Yesterday's charges (not collections, charges)
-
Appointment fill rate
-
Service mix percentage (procedures vs. visits)
Cost indicators:
-
Staff hours worked vs. scheduled
-
Supply usage variance
-
Overtime hours triggered
Efficiency indicators:
-
Revenue per provider hour
-
Patients seen per support staff hour
-
No-show impact in dollars
Post these numbers where everyone sees them. Not buried in emails or hidden in management offices — visible to all staff. When the medical assistants understand that today's no-shows cost $1,200 in lost margin, they take confirmation calls more seriously.
A pediatric practice in Florida started posting daily margin indicators on a whiteboard by the time clock. Nothing fancy, just three numbers: yesterday's margin estimate, this week's trend, this month's projection. Staff started self-organizing to protect margins. The front desk began calling no-show risks proactively. Medical assistants started managing supply usage more carefully. Providers started arriving on time to avoid schedule compression.
The behavioral change matters more than the precision. Your daily margin estimate might be off by 10-15%. That's fine. The point is creating awareness and urgency around financial performance before problems compound.
Connecting this to your monthly KPI system, these daily indicators should feed into your triggered actions. When daily margins drop below threshold for three consecutive days, that triggers specific operational responses — not panic, but predetermined adjustments that restore performance.
The reality of operating through inflation cycles
Inflation isn't just about higher costs — it fundamentally changes how clinics need to operate. The practices that thrive during these periods don't just cut costs or demand higher reimbursements. They build operational flexibility that lets them adjust quickly without breaking core patient care.
These changes aren't temporary inflation responses. They're operational improvements that happen to be especially critical during inflationary periods. Variable-rate scheduling improves revenue whether inflation is 2% or 5%. Billing velocity helps cash flow in any economic environment. Flexible staffing pools reduce burnout regardless of wage pressures.
What makes them essential now is that inflation removes your margin for error. The inefficiencies you could tolerate when supplies cost 10% less and staff expected 2% annual raises become existential threats when everything costs more and revenue stays flat.
The clinics succeeding share three characteristics. First, they measure everything that matters daily, not monthly. They know their margin trajectory before it shows up in P&L statements. They spot problems while they're still solvable.
Second, they've built systematic responses to common problems. No-shows, staffing gaps, denial risks — these have predetermined solutions that trigger automatically based on data, not feelings.
Third, they've embraced operational flexibility over rigid structure. Their scheduling adapts to demand. Their staffing adjusts to volume. Their processes evolve based on results.
The inflationary pressure won't last forever. But the operational discipline you build navigating it will serve you through whatever comes next. The clinics that use this crisis to build better operations will emerge stronger. Those that simply try to wait it out may not emerge at all.
Making these changes without breaking ongoing operations
The biggest mistake is clinics trying to implement all these changes simultaneously. Your staff is already stressed from inflation pressures. Adding five major operational changes at once guarantees failure.
Start with billing velocity. It provides immediate cash flow relief and requires minimal workflow disruption. Track submission speed for one week, identify the bottlenecks, fix the biggest one. Once that's stable, add daily margin visibility.
The scheduling and staffing changes require more planning. Build the frameworks first, test with small groups, then expand. A partial implementation that works beats a comprehensive plan that fails.
Remember, the goal isn't perfection. It's building enough operational efficiency to maintain margins while inflation runs its course. Every small improvement compounds. A 5% reduction in no-shows, 10% improvement in billing velocity, and 8% decrease in overtime costs might not sound dramatic individually. Together, they're the difference between surviving and closing.
The clinics that make it through this period won't be the ones with the most resources. They'll be the ones that adapted fastest, measured consistently, and executed systematically despite the chaos around them.
Ready to transform your practice workflow?
Join 2,000+ healthcare providers using GoCliny to increase efficiency, improve patient satisfaction, and grow revenue.