

Healthcare practices bleed revenue through appointment chaos, but not where you'd expect. The damage happens between systems—when your front desk doesn't know a patient has already rescheduled three times, when billing misses that insurance verification expired during a reschedule chain, when providers show up to empty slots because nobody updated the master schedule.
Most practices attack this wrong. They buy better scheduling software, train staff on phone etiquette, send more reminder texts. The underlying operational structure stays broken. You need an appointment lifecycle system with clear stages, handoff protocols, and escalation triggers that eliminate the constant manual scrambling.
The appointment lifecycle breaks at predictable points
When a patient calls to schedule, what actually happens? Not the ideal version—the real version.
Your scheduler checks the system, finds an opening, books it. Simple enough. But that appointment now exists in multiple parallel universes. It's in your practice management system as a scheduled slot. It's in your provider's mental calendar as expected revenue. It's in your billing system as a future claim. It's in your clinical workflow as prep work needed.
Each reschedule creates ripple effects across all these systems. A Tuesday morning slot moves to Thursday afternoon—your MA needs to prep different materials, your biller needs to reverify benefits because it crosses into a new week, your provider loses a high-reimbursement morning slot for a lower afternoon rate.
Without a structured lifecycle, these changes happen through informal communication. Sticky notes. Quick hallway conversations. "Hey, don't forget that Johnson moved to Thursday." The manual coordination compounds until your team spends more time managing schedule changes than seeing patients.
This is where operational software with AI automation becomes essential. Instead of relying on informal communication, automated systems can track appointment changes across all platforms simultaneously, triggering necessary updates to clinical prep, billing verification, and provider schedules without manual intervention.
Why traditional approaches fail at scale
Small practices survive on tribal knowledge. When you've got one provider and two staff members, everyone knows everything. Martha at the front desk knows Mr. Peterson always reschedules his first appointment. She mentally tracks it, follows up appropriately, makes it work.
Eliminate appointment gaps and no-shows.
GoCliny streamlines every patient interaction from booking to billing—seamlessly.
- Unified appointment scheduling
- Automated patient reminders
- Staff calendar & task management
No credit card required
Scale to three providers and twelve staff members, and Martha's mental system collapses. The new scheduler doesn't know Mr. Peterson's pattern. The float receptionist covering lunch doesn't know to check the paper note about his insurance change. The afternoon billing clerk doesn't know this is his fourth reschedule and needs a different protocol.
Practices typically respond by adding more communication layers. Morning huddles become 45-minute scheduling reviews. Email chains multiply. Slack channels overflow with "FYI, Williams moved to next week" messages. You're adding complexity to manage complexity.
The solution isn't more communication—it's structured handoffs with clear ownership at each lifecycle stage.
Mapping your appointment lifecycle stages
Identify what actually happens to an appointment from initial request to claim payment. Not what should happen—what does happen in your practice right now.
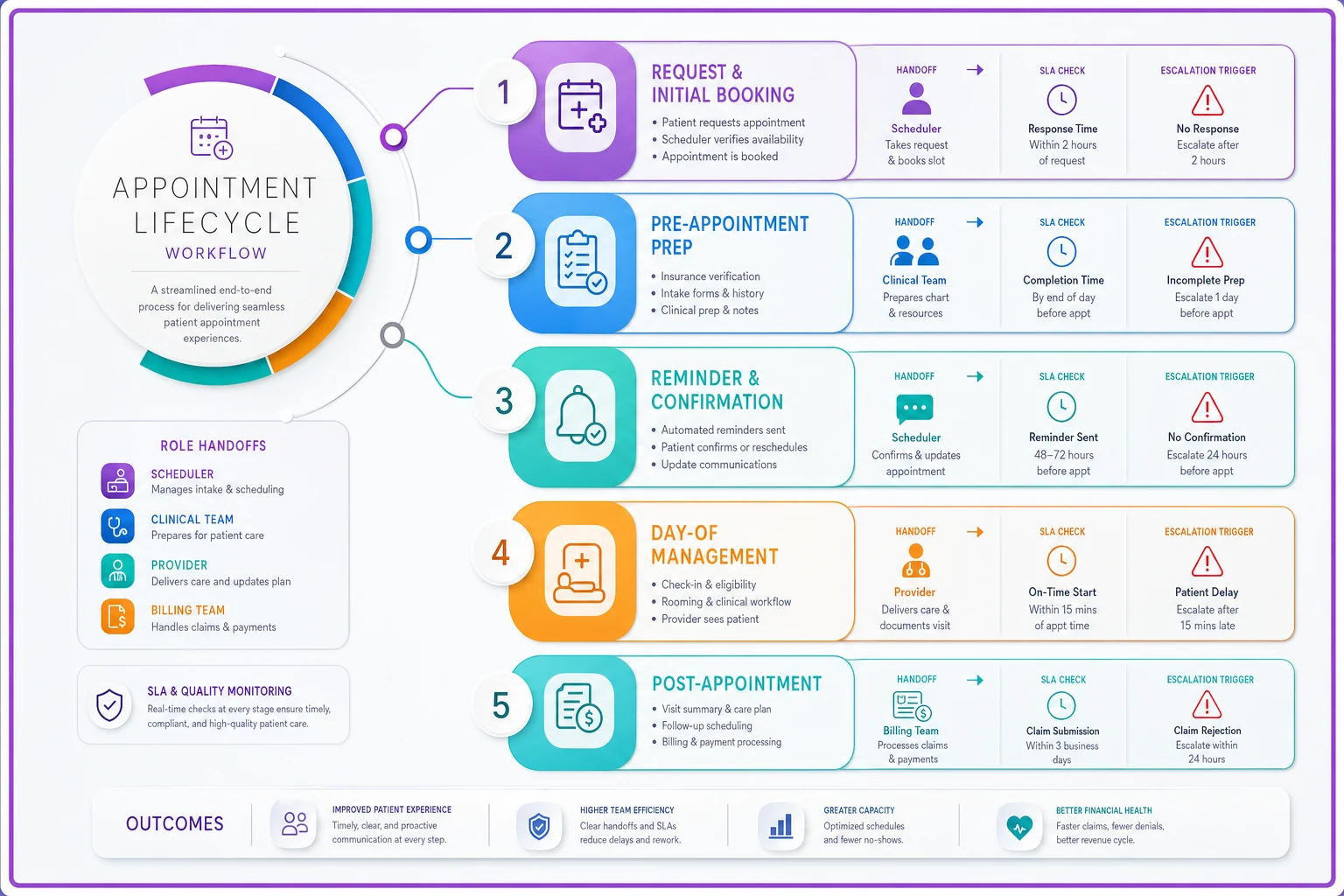
Here's a common stage breakdown:
-
Stage 1
Request and Initial Booking
- Patient calls or requests online - Scheduler checks availability - Basic insurance verification - Appointment booked in system - Confirmation sent -
Stage 2
Pre-Appointment Prep
- Insurance authorization (if needed) - Clinical prep requirements identified - Provider preferences checked - Prior records pulled -
Stage 3
Reminder and Confirmation
- Automated reminder sent - Response logged - No-response protocol triggered - Same-day confirmation -
Stage 4
Day-of Management
- Check-in process - Insurance verification - Copay collection - Clinical handoff -
Stage 5
Post-Appointment
- Checkout and follow-up scheduling - Claim submission - Payment posting - Patient communication
Each stage needs an owner, not just a person who handles it sometimes. The owner doesn't do all the work—they ensure the work happens and catch failures.
Your stages might be different. Some practices combine prep and reminder. Others split day-of management into separate check-in and clinical phases. Map what actually exists, then improve it.
Building SLAs that actually work
Service Level Agreements sound corporate, but they're really just promises about timing and handoffs. Without them, everything becomes urgent and nothing gets done properly.
-
Initial callback
within 2 business hours during office hours
-
Insurance verification
completed within 24 hours of booking
-
Prior auth submission
within 48 hours if appointment is 7+ days out
-
Patient prep instructions sent
72 hours before appointment
-
Day-before confirmation
by 4 PM the business day before
But timing matters less than what happens when you miss them.
A patient calls at 3 PM Friday for a Monday appointment. Your 24-hour insurance verification SLA is already blown. Does the scheduler stay late? Does Monday morning staff handle it? Who makes that decision?
Build escalation triggers directly into your SLAs:
-
Hour 20-24
Scheduler sends priority flag to billing
-
Hour 24+
Auto-escalate to practice manager
-
Hour 36+
Provider notified of potential same-day verification
Assign clear escalation owners so SLA misses route automatically to the person empowered to act.
The escalation isn't punishment—it's operational clarity. Everyone knows what happens when things slip.
The reschedule cascade problem
Most practices completely fall apart here. A patient reschedules, and suddenly you're playing telephone across six departments.
Monday 2 PM - Patient calls to move Thursday appointment to next week Monday 2:15 PM - Scheduler moves appointment in system Monday 4 PM - Provider still expects Thursday patient (not notified) Tuesday 9 AM - MA preps Thursday materials (not notified) Wednesday 3 PM - Billing reverifies for wrong date Thursday 8 AM - Provider discovers empty slot Thursday 8:15 AM - Scramble to fill slot or lose revenue
One reschedule, six failure points. Multiply by the 15-20% of appointments that reschedule weekly.
Your lifecycle system needs explicit reschedule protocols:
-
Scheduler updates primary system
-
Auto-notification to provider (same day)
-
Auto-notification to clinical prep (same day)
-
Auto-flag for insurance reverification
-
Auto-add to "fill list" for original slot
-
Auto-trigger new reminder sequence
Notice "auto" appears frequently. Manual notifications fail. Always.
Sample SOP for complex appointment types
Different appointment types need different lifecycle rules. A new patient consultation has different requirements than a routine follow-up. Build separate SOPs for your main appointment categories.
New Specialty Consultation SOP
-
Booking Phase (Day 0) - Capture referring provider info - Verify insurance eligibility - Check prior auth requirements - Schedule 60-minute slot - Send new patient packet
-
Verification Phase (Day 1-2) - Complete insurance verification - Submit prior auth if needed - Confirm referring provider records received - Flag any coverage issues
-
Prep Phase (Day 3-7) - Clinical team reviews referral - Provider previews case - Special equipment confirmed - Interpreter services arranged if needed
-
Confirmation Phase (Day 6-7) - First reminder sent - Packet completion checked - Transportation confirmed - Day-before confirmation call
-
Day-of Phase - Early arrival for paperwork - Insurance card scanned - Copay collected - Clinical intake completed
-
Handoff Triggers - No insurance response by Day 2
Escalate to billing manager - No packet by Day 5: Outreach call required - No confirmation response: Morning-of call required - No show: Same-day reschedule attempt
The SOP isn't micromanagement—it's clarity when chaos hits.
Creating escalation paths that don't annoy everyone
Escalation without context creates alert fatigue. Your practice manager doesn't need to know about every minor delay. But they absolutely need to know when patterns emerge.
Build smart escalation triggers:
-
Single SLA miss
Team lead notified
-
Multiple SLA misses same patient
Manager notified
-
Critical SLA miss (same-day issues)
Immediate escalation
Make escalation informational, not punitive. You're identifying system failures, not people failures.
-
Same SLA missed 3x in one week
Process review triggered
-
Same staff member missing SLAs
Training review triggered
-
Same appointment type consistently problematic
Workflow revision triggered
Make escalation informational, not punitive. You're identifying system failures, not people failures.
KPIs that reveal system health
Most practices track appointment volume and no-show rates. That's like tracking your car's speed but not checking the engine temperature. You need operational KPIs that show system health:
| Metric Category | Key Indicators |
|---|---|
| Lifecycle Efficiency | Time from request to booking, Percentage requiring escalation, Reschedule cascade completion rate |
| Quality Indicators | Patient arriving without completed paperwork, Insurance issues discovered day-of, Provider schedule gaps |
| Revenue Impact | Revenue lost to unfilled reschedule slots, Collections delayed by verification failures, Patient leakage after reschedule friction |
Start tracking three of these. You'll immediately see where your lifecycle breaks down.
The technology stack that enables this
Manual lifecycle management is impossible at scale. You need systems that create automatic handoffs and track SLA compliance without constant human monitoring.
-
Scheduling system with workflow triggers
-
Communication platform with automatic escalation
-
Document management with version control
-
Reporting dashboard for KPI tracking
The integration matters more than the individual tools. If your scheduler has to manually notify billing about every insurance check, the system fails. If providers can't see real-time schedule changes, the system fails.
Modern AI-powered operational software can orchestrate these handoffs automatically. When a patient reschedules, the system immediately triggers insurance reverification, notifies all stakeholders, updates prep requirements, and adds the original slot to your fill list. No sticky notes, no email chains, no forgotten notifications.
The AI components handle the complex decision trees—if this patient has Medicare and they're rescheduling to next month, trigger new authorization. If this provider prefers 15-minute buffers between complex cases, don't allow back-to-back booking. If this is the third reschedule, require manager approval.
That automation layer eliminates the manual coordination that kills productivity. Your team stops chasing information and starts managing patients.
Building team buy-in for lifecycle management
Your front desk team thinks you're adding bureaucracy. Your providers think you're overcomplicating scheduling. Your billing team is already overwhelmed.
Start with a single appointment type. Pick your most problematic one—probably new patient consultations or procedures requiring authorization. Build the lifecycle for just that type. Run it for a month. Document the improvements.
-
One appointment type
-
Add reschedule protocols
-
Add escalation triggers
-
Expand to next appointment type
-
Integrate automation tools
-
Full lifecycle deployment
Each phase should take 2-3 weeks. Don't rush—broken processes implemented quickly just fail faster.
Common failure points and how to avoid them
Failure: Over-engineering the lifecycle You map 47 steps for a routine follow-up. Your team ignores the system entirely.
Solution: Start with 5-7 major stages maximum. Add substeps only where failures actually occur.
Failure: Rigid SLAs that ignore reality Your SLA says 2-hour callback, but lunch rush makes that impossible.
Solution: Build conditional SLAs. "2 hours during normal volume, 4 hours during peak times (11 AM - 2 PM)."
Failure: No accountability for stage ownership Everyone's responsible, so no one's responsible.
Solution: Name actual people. "Jennifer owns Stage 2 verification. When Jennifer's out, Michael owns it." Clear, specific, tracked.
Failure: Manual tracking of compliance You expect staff to self-report when they miss SLAs.
Solution: Automatic tracking or it doesn't happen. Your system should generate compliance reports, not rely on human reporting.
These aren't the only ways to fail, but they're the most common. Build the system, then adapt it to your reality.
Sample timing rules for different practice types
Here are sample timing rules you can use as starting points for different practice types.
-
Primary Care Practice - New patient booking
Same day response - Verification: Within 24 hours - Reminder: 48 hours prior - Confirmation: Morning of - Reschedule: Within 2 hours notification
-
Specialty Surgery Practice - Consultation booking
Within 4 hours - Prior auth: Within 72 hours - Prep instructions: 1 week prior - Final confirmation: 48 hours prior - Reschedule: Requires 72-hour notice
-
Mental Health Practice - Initial intake
Within same business day - Insurance verification: Before first appointment - Reminder: 24 hours prior - Confirmation: Not required (reduces anxiety) - Reschedule: Immediate availability check for continuity
-
Multi-Specialty Clinic - Triage to appropriate specialty
Within 2 hours - Coordinator assignment: Based on complexity - Verification: Varies by service - Prep: Customized by department - Reschedule: Central coordination required
Your timing will be different. Use these as starting points, not gospel.
The real ROI of appointment lifecycle management
Practices lose around $150 per unfilled slot. If you're averaging 20 providers seeing 20 patients daily, with 15% last-minute changes, you're looking at 60 schedule disruptions daily. Even if you only lose revenue on 10% of those, that's $900 daily in direct losses.
The hidden costs hurt more. Your scheduler spending 3 hours daily on reschedule coordination at $25/hour. Your billing team working overtime to reverify insurance. Your providers' frustration when their carefully planned day falls apart. Your patients' irritation when no one seems to know about their appointment details.
A structured lifecycle eliminates these friction costs. Not through better people or more effort—through better systems.
One multi-location practice implemented lifecycle management across their 4 clinics. Their unfilled slot rate dropped from around 12% to 4% within three months. Their staff overtime for schedule management went from 45 hours weekly to under 10. Their patient satisfaction scores jumped because appointments felt organized, not chaotic.
The numbers matter, but the operational sanity matters more. When your team stops constantly scrambling to fix schedule problems, they can focus on patients instead of logistics.
Getting started next week
Don't redesign your entire appointment system. Start here:
Pick your worst appointment problem. Maybe it's new patients no-showing. Maybe it's procedures getting rescheduled multiple times. Maybe it's insurance surprises day-of.
-
Booking
-
Verification
-
Prep
-
Day-of
-
Follow-up
Identify who owns each stage. Create one SLA for each stage. Build one escalation trigger.
Run this micro-lifecycle for two weeks. Track what breaks. Adjust the timing. Add automation where manual handoffs fail.
Then expand gradually. Add your next problematic appointment type. Integrate your communication tools. Build in automatic notifications.
Within 90 days, you'll have eliminated most manual rescheduling chaos. Your team will stop playing phone tag about schedule changes. Your providers will trust that their schedule reflects reality. Your patients will experience a practice that actually has its operations together.
The appointment lifecycle isn't about perfection—it's about predictability. When everyone knows what happens at each stage, who owns each handoff, and when escalation triggers, the constant scramble disappears. You stop managing crises and start managing a system.
That's when healthcare operations actually work. Not through heroic effort or perfect staff, but through structured processes that treat appointments as workflows, not isolated events. Build the lifecycle, and the chaos resolves itself.
Ready to transform your practice workflow?
Join 2,000+ healthcare providers using GoCliny to increase efficiency, improve patient satisfaction, and grow revenue.