
Three months ago, a 6-provider orthopedic clinic in Atlanta discovered $147,000 sitting in unworked denials. Not because they lacked staff—they had four people handling revenue cycle. The problem? Their front desk collected insurance cards without verifying benefits, their MAs coded encounters wrong about 30% of the time, and their billing team spent most days putting out fires instead of working claims systematically.
This wasn't incompetence. It was a broken revenue cycle framework where nobody owned the whole process.
Building operational software for healthcare practices—solo psychiatry to 20-provider urgent care chains—the same pattern emerges everywhere. Clinics treat revenue cycle like separate departments instead of one continuous workflow. Front desk thinks their job ends when the patient sits down. Clinical staff assumes billing happens automatically. Billing feels stuck cleaning up everyone else's mess.
The clinics that actually collect what they bill? They run revenue cycle as one integrated operation with clear handoffs, ownership at each stage, and specific playbooks when things go wrong.
Why traditional RCM training misses the operational reality
Most revenue cycle training focuses on coding accuracy and payer rules. That's like teaching traffic laws without explaining how to drive.
Real revenue cycle operations start way before the claim gets submitted. They start when Sarah calls to schedule her knee evaluation and your front desk either captures the right information or sets up a denial three weeks later.
Practices hire expensive RCM consultants who deliver 200-page manuals nobody reads. Meanwhile, their front desk still doesn't know what to do when a patient shows up with out-of-network insurance. Clinical staff still picks CPT codes based on gut feeling. Billing teams still work claims oldest-first instead of highest-value-first.
A functional revenue cycle framework connects every person who touches the patient journey to the money that eventually arrives. Your receptionist understands how one missing data field creates downstream chaos. Your MAs know which documentation triggers automatic denials. Your billing team has clear escalation paths instead of endless "follow-ups."
The five stages where money actually gets lost
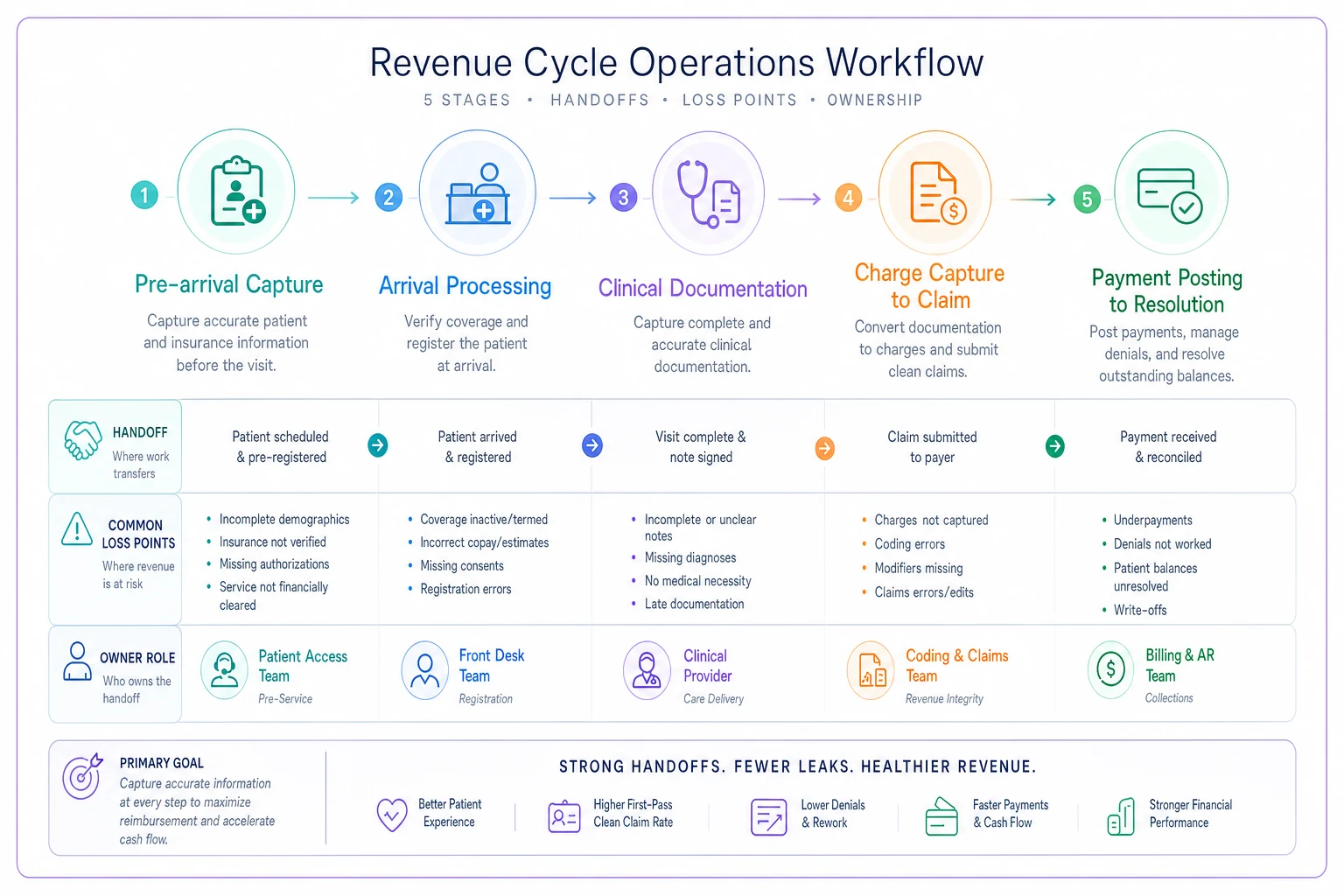
Forget the textbook flowchart with 47 steps. Money disappears at five specific handoff points:
Eliminate appointment gaps and no-shows.
GoCliny streamlines every patient interaction from booking to billing—seamlessly.
- Unified appointment scheduling
- Automated patient reminders
- Staff calendar & task management
No credit card required
Stage 1: Pre-arrival capture Everything from appointment scheduling through day-before confirmation. Money gets lost when insurance details are wrong, authorizations are missed, or copays aren't identified. A dermatology practice discovered 40% of their new patient appointments had insurance typos that caused instant rejections.
Stage 2: Arrival processing The eight minutes between parking lot and exam room. Clinics lose money through missed demographic updates, skipped financial agreements, and forgotten copay collection. One urgent care was leaving roughly $2,100 weekly on the table just from inconsistent copay collection.
Stage 3: Clinical documentation From rooming through checkout. Diagnosis codes get missed, procedures go undocumented, and modifiers get forgotten. An internal medicine group found their providers were undercoding preventive visits as sick visits about 25% of the time—roughly $64,000 annual loss.
Stage 4: Charge capture to claim The 24-48 hours after the visit. Money evaporates through missing charges, incorrect bundling, and delayed submission. Claims submitted after day 3 get denied 3x more often than same-day submissions.
Stage 5: Payment posting to resolution Everything after the claim goes out. Denials pile up, patient balances get ignored, and appeals die in someone's inbox. Most practices work denials first-in-first-out when they should work highest-value-first with strict timelines.
This workflow diagram illustrates the five stages, handoffs, common loss points, and where owners should sit in the process.
Each stage needs an owner. Not a department—a specific person whose job performance depends on that stage functioning correctly.
Ownership matrix that actually works in small practices
Big hospital systems can afford dedicated teams for each revenue cycle function. Your 8-provider family medicine practice can't. The same person checking insurance might also room patients and answer phones.
Here's an ownership structure that works with limited staff:
Front Desk Lead owns Stages 1-2:
-
Verification accuracy rate (target
>95%)
-
Time to verify benefits (target
<24hrs before appointment)
-
Copay collection rate (target
>90%)
-
Registration completeness (target
100% by rooming)
Clinical Supervisor owns Stage 3:
-
Documentation completion time (target
same day)
-
Coding accuracy by provider (target
>92%)
-
Unsigned note percentage (target
<5%)
-
Charge lag days (target
<1)
Billing Lead owns Stages 4-5:
-
Clean claim rate (target
>90%)
-
Days in AR (target
<35)
-
Denial rate (target
<8%)
-
Resolution velocity (target
first touch within 48hrs)
| Role | Metrics |
|---|---|
| Front Desk Lead | Verification accuracy rate (target: >95%); Time to verify benefits (target: <24hrs before appointment); Copay collection rate (target: >90%); Registration completeness (target: 100% by rooming) |
| Clinical Supervisor | Documentation completion time (target: same day); Coding accuracy by provider (target: >92%); Unsigned note percentage (target: <5%); Charge lag days (target: <1) |
| Billing Lead | Clean claim rate (target: >90%); Days in AR (target: <35); Denial rate (target: <8%); Resolution velocity (target: first touch within 48hrs) |
The trick isn't just assigning ownership—it's giving owners actual authority to fix problems. Your Front Desk Lead needs power to change verification workflows. Your Clinical Supervisor needs ability to require provider training. Your Billing Lead needs authority to escalate payer issues.
Give owners the authority to fix problems—ownership without authority becomes blame.
Without authority, ownership becomes blame without solutions.
SLAs that prevent the "we'll look into it" black hole
Service Level Agreements sound corporate, but they're really just promises about timing. When a claim gets denied, how fast does someone touch it? When insurance changes, how quickly is it updated?
Insurance Verification SLA:
-
New patients
verified within 2 hours of scheduling
-
Existing patients
reverified if last check >30 days
-
Walk-ins
verified before rooming
-
Changes discovered at check-in
updated before claim submission
Documentation SLA:
-
Visit notes
signed within 4 hours
-
Procedure notes
completed same day
-
Missing documentation requests
responded within 24 hours
-
Coding queries
answered by next business day
Charge Entry SLA:
-
Standard visits
charged within 24 hours
-
Procedures
charged within 48 hours
-
Hospital/facility charges
captured within 72 hours
-
Missing charge reports
reviewed daily
Denial Management SLA:
-
Initial review
within 2 business days
-
Missing information requests
submitted within 5 days
-
Appeals
filed within payer deadline minus 10 days
-
Write-off decisions
approved monthly, not quarterly
A cardiology practice implemented these SLAs and watched their over-90-day AR drop from $124,000 to around $31,000 in four months. Not through better software or more staff—just clear expectations about timing.
Failure mode playbooks for the disasters that definitely will happen
Every clinic thinks their problems are unique. They're not. The same dozen failures happen everywhere, just with different payer names and software systems.
Document the fix once and follow it forever:
Playbook: Mass denial from payer system change
Trigger: More than 10 claims from same payer denied with same error
Immediate actions:
-
Stop submitting claims to that payer
-
Call provider relations (not standard customer service)
-
Document system error and reference number
-
Flag all pending claims for hold
Resolution path:
-
Resubmit with corrected format once confirmed
-
Appeal all denials with system error documentation
-
Track lost interest for contracts negotiation
Playbook: Provider credentialing lapse
Trigger: Claims denied for "provider not credentialed" or "out of network"
Immediate actions:
-
Verify credentialing status directly with payer
-
Stop scheduling new patients with that insurance
-
Identify all affected claims in pipeline
-
Notify patients about potential balance responsibility
Resolution path:
-
Fast-track recredentialing with expedite request
-
Hold claims if within timely filing
-
Negotiate retroactive effective date
-
Consider single-case agreements for active treatments
Playbook: Prior authorization expiration cascade
Trigger: Multiple visits denied for "no authorization"
Immediate actions:
-
Pull report of all current authorizations
-
Identify expiring within 30 days
-
Stop scheduling beyond auth end dates
-
Create renewal tracking spreadsheet
Resolution path:
-
Submit renewals 45 days before expiration
-
Build auth tracking into scheduling system
-
Assign auth ownership to specific role
-
Create patient notification template
Playbook: Wrong insurance on file
Trigger: Claim rejected for "patient not found" or "coverage terminated"
Immediate actions:
-
Call patient before working claim
-
Check employer website for plan changes
-
Verify with eligibility tool
-
Update all family members simultaneously
Resolution path:
-
Resubmit to correct payer
-
Calculate timely filing deadline
-
Set reminder for secondary billing if needed
-
Flag for registration retraining if pattern emerges
Document the fix once and follow it forever:
Dashboard metrics that trigger action, not just reports
Most practice dashboards show vanity metrics. Total charges. Gross collection rate. Average days in AR. These tell you what happened, not what to do about it.
Daily Flash Metrics:
-
Unworked claims >5 days old (action
assign immediately)
-
Eligibility failures at check-in (action
reverify before rooming)
-
Unsigned notes >24 hours (action
provider reminder)
-
Posted payments unmatched (action
research before deposit)
Weekly Trend Metrics:
-
Denial rate by category (action
fix process causing spike)
-
Collection rate by payer (action
investigate drops >5%)
-
Charge lag by provider (action
training if >2 days)
-
Prior auth turnaround (action
escalate if >5 days)
Monthly Strategic Metrics:
-
Revenue per encounter by payer (action
renegotiate low performers)
-
Write-off percentage by reason (action
address systematic issues)
-
Patient balance >90 days (action
payment plan or collections)
-
Clean claim rate by registration staff (action
targeted training)
A multispecialty group in Denver built this dashboard structure and discovered their afternoon front desk person had a 60% eligibility error rate—she'd been guessing at insurance details instead of verifying. Fixed with two hours of training, worth about $18,000 monthly in prevented denials.
How AI automation transforms firefighting into systematic operations
The operational challenge with revenue cycle isn't that people don't know what to do—it's that manual workflows break down under volume. When your biller has 200 claims to work, they can't carefully review each one. When your front desk has a line of patients, they skip verification steps.
AI-powered operational software changes this dynamic entirely. Not by replacing people, but by automating the repetitive checks that humans skip when busy.
Modern revenue cycle platforms with AI automation handle the mundane validation that causes downstream disasters. They verify insurance in the background while your front desk handles patients. They flag documentation gaps before claims go out. They prioritize denials by value and deadline, not just age.
That orthopedic clinic I mentioned? They implemented an AI-assisted RCM platform that automatically verified benefits for every appointment, flagged missing authorizations 48 hours before visits, and categorized denials by fixability. Their $147,000 in unworked denials dropped to under $20,000 within 90 days.
But the real transformation wasn't the technology—it was that their team could finally focus on exceptions instead of routine tasks. Their billing team spent time on complex appeals instead of chasing missing demographics. Their front desk built patient relationships instead of making verification calls.
AI agents in revenue cycle operations excel at the pattern recognition that humans find exhausting. They spot when a payer suddenly changes claim requirements. They identify providers who consistently use wrong modifiers. They predict which claims will deny based on historical patterns and flag them for prevention.
The key is viewing AI automation as operational infrastructure, not magic. It needs clear workflows to follow, consistent data to analyze, and human oversight for exceptions. But when implemented properly, it transforms revenue cycle from daily crisis management into predictable operations.
Stop treating revenue cycle like someone else's problem
Revenue cycle struggles are rarely about coding knowledge or payer expertise. They're about treating revenue cycle like a hot potato nobody wants to hold.
Your front desk thinks billing is billing's problem. Billing thinks documentation is clinical's problem. Clinical thinks insurance is front desk's problem. Meanwhile, money hemorrhages at every handoff point.
The clinics that actually collect what they're owed run revenue cycle as one integrated operation. Every staff member understands how their actions affect collections. Clear ownership prevents finger-pointing. Documented playbooks eliminate panic. Real-time dashboards drive action instead of meetings.
Most importantly, they've accepted that revenue cycle excellence isn't about perfection—it's about systematic improvement. Every denied claim teaches something. Every workflow breakdown becomes a playbook. Every metric drives specific behavior change.
This framework—discrete stages, owner accountability, concrete SLAs, failure playbooks, and action-triggering dashboards—works because it acknowledges operational reality. People make mistakes. Systems break. Payers change rules. But with the right structure, these become manageable hiccups instead of financial disasters.
Your revenue cycle doesn't need another consultant's manual or coding seminar. It needs operational infrastructure that connects front-desk actions to back-office outcomes. It needs owners who can actually fix problems, not just report them. It needs playbooks for real failures, not theoretical edge cases.
Build this framework, and watch your revenue cycle transform from a mystery into a machine. One that actually pays you for the work you do.
Ready to transform your practice workflow?
Join 2,000+ healthcare providers using GoCliny to increase efficiency, improve patient satisfaction, and grow revenue.